Introduction
Chapter 2 established that the structure of human experience is decomposable: altering specific neural structures alters specific aspects of what a person sees, feels, thinks, and wants while leaving other aspects intact. That fact - graded, specific, and replicable across more than a century of clinical, pharmacological, and stimulation evidence - is what permits a framework that breaks experience into a finite set of independent dimensions rather than treating it as an indivisible whole. Chapter 2 also introduced a vector architecture: V0 (physical stimulus), Vc (content representation), Vn (neural state), Ve (experiential state), and Vp (behavioral output). One vector in that architecture - Ve - was given an initial operating set of five dimensions (valence, arousal, dominance, novelty, engagement) but explicitly flagged as incomplete. This chapter replaces that placeholder with a full decomposition grounded in elimination evidence.
Chapter 3 inventoried the hardware that produces experience: ten receptor systems, seven cortical networks, subcortical structures, and six neurochemical systems. It classified each as state producer, modulator, or infrastructure (Classification, Tool 5), and assigned confidence tiers - higher confidence for cortical-surface systems readable by brain encoding models, lower confidence for subcortical systems that those models cannot directly reach. This chapter maps the experiential dimensions onto that hardware inventory: every dimension named here has a producing structure from Chapter 3’s catalog, and inherits that structure’s confidence tier.
This chapter does the work those foundations license. It walks through each dimension at three resolutions and shows the evidence that earns its place. A reader should be able to ask, of every dimension named here, “what experiment shows that this is separable from the others?” - and the chapter aims to provide the answer in the same paragraph.
A constraint applies throughout. The chapter operates entirely within what Chapter 2 called Scope A of Experience Space - the structurally inferable region. Scope A covers the dimensions themselves, their independence, their nesting, and their gradedness. Scope B - the qualitative character of experience, what red looks like, what longing feels like - is acknowledged as real but not characterized here. The methods this chapter uses (lesion, dissociation, stimulation, pharmacological manipulation) recover structure, not subjective quality. When a patient with bilateral primary visual cortex damage loses vision, we learn that vision is structurally separable from hearing, emotion, and cognition. We do not learn what it was like to see. The first kind of knowledge is what the Khozai framework needs.
What this does NOT say. This chapter does not claim that the dimension set is final or complete - it is the best-supported decomposition the evidence currently yields, and it grows with evidence. It does not characterize Scope B (qualitative character). It does not claim that every dimension is equally readable by brain encoding models - some dimensions sit in cortical structures that TRIBE v2 can predict (higher confidence), while others sit in subcortical structures it cannot directly reach (lower confidence). The chapter names both kinds and states which is which.
Each chapter stands on its own terminology. Technical terms used in Chapter 2 are reintroduced here on first appearance with a plain-language gloss in the same sentence.
1. Method
The dimensions named in this chapter are not the result of philosophical argument. They are the result of one repeated experiment: damage a part of the brain and observe what specifically disappears from a person’s experience. When some aspect of what a person perceives or feels is gone after the damage, but other aspects remain intact, that aspect is separable. When the same aspect can be eliminated by damage to one structure and preserved under damage to another, the aspect is independent. Stack enough of these results together and the architecture of experience becomes visible - not because anyone designed it that way, but because biology imposed it.
This method is selective elimination, the procedure named in Chapter 2 as Premise 5: altering specific neural structures alters specific aspects of experience while leaving others intact. It is the primary tool of this chapter, and it is applied using four formal tests introduced in Chapter 2’s toolkit. The method has real critics: the psychologists John Dunn and Kim Kirsner [34] argued that a single underlying system with different processing demands can mimic both single and double dissociations. Chapter 2 addressed this by requiring double dissociation as the gold standard and treating inferred independence as an empirical hypothesis subject to revision. This chapter’s use of the method is subject to those limitations.
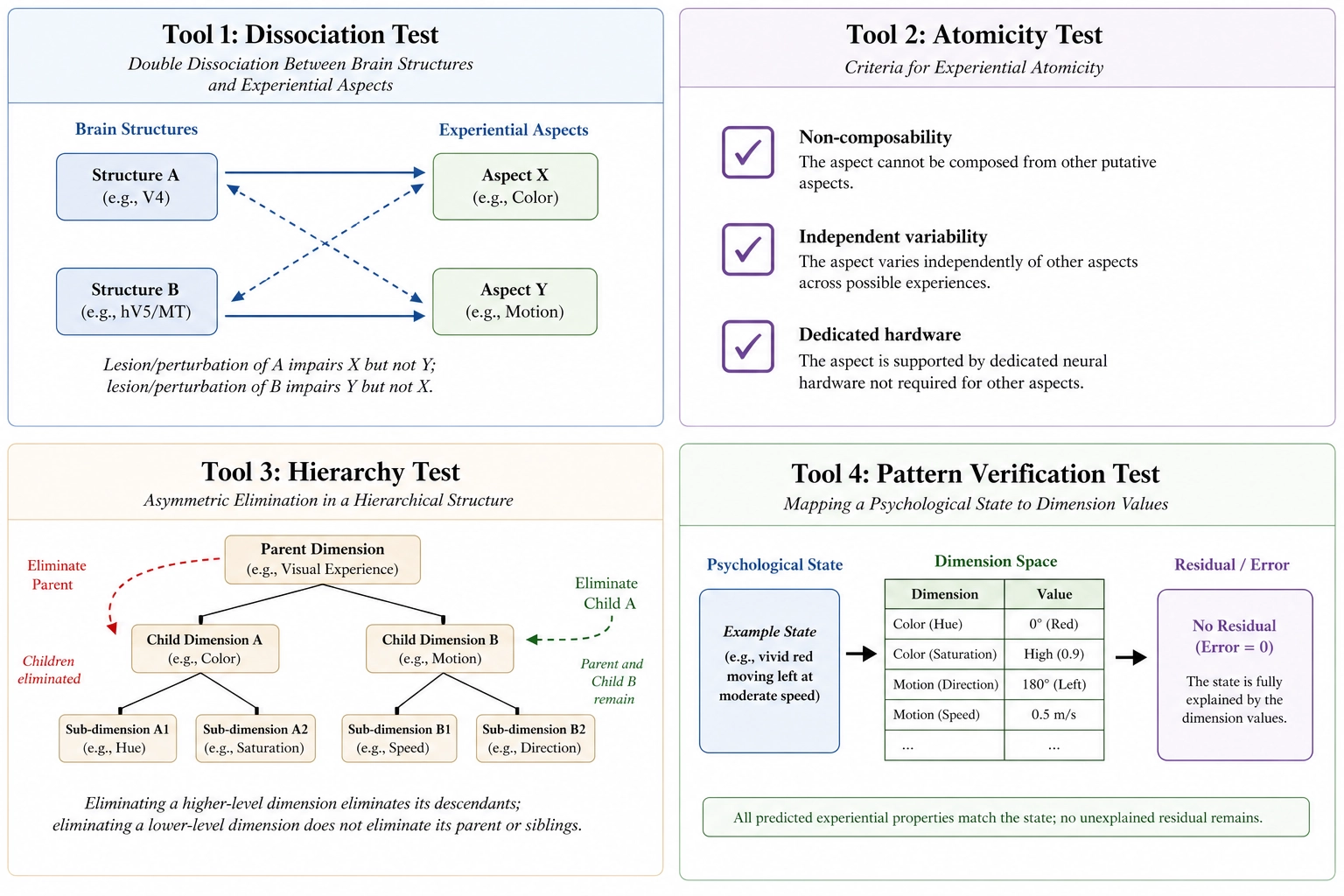
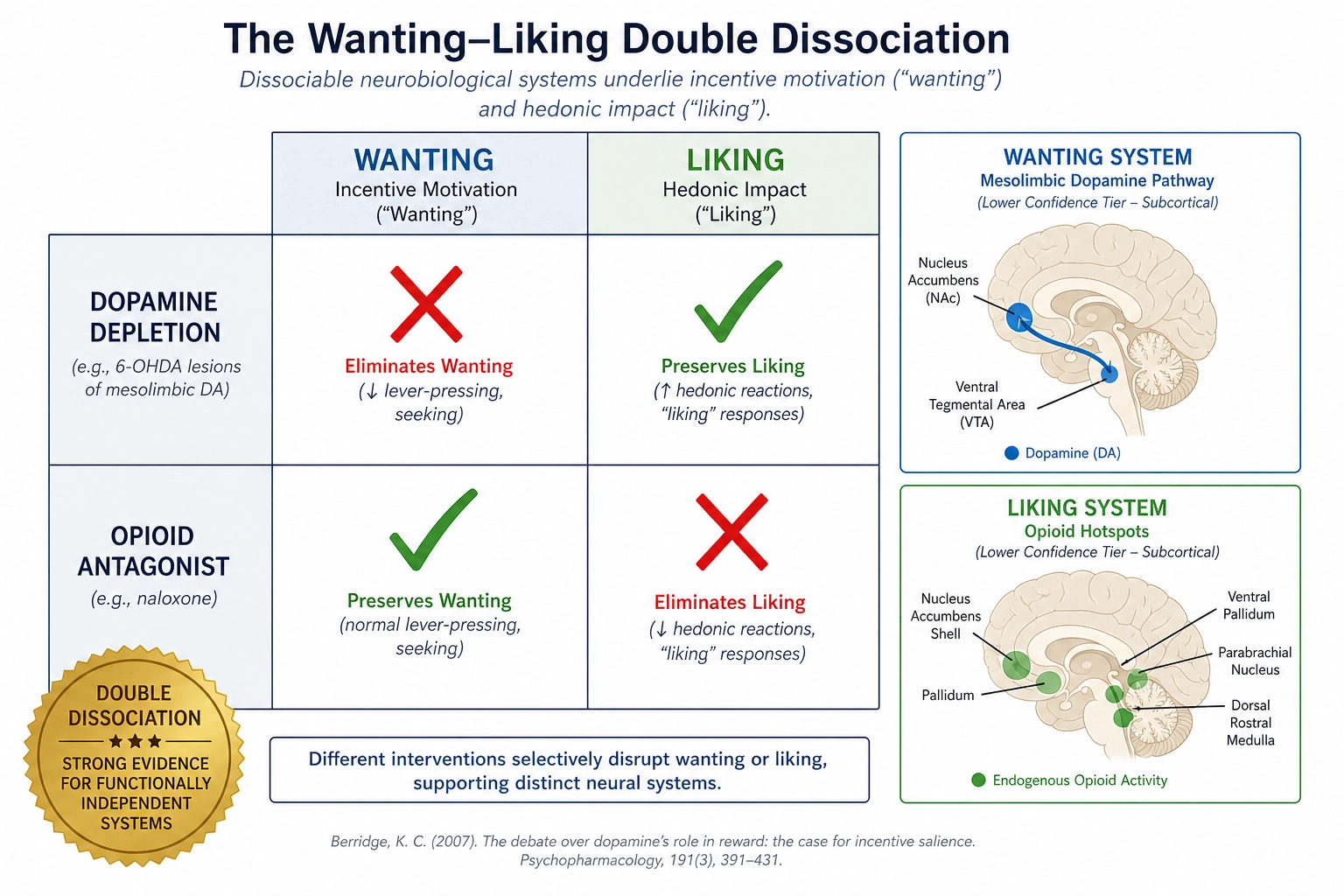
Tool 1: the Dissociation Test. This test answers whether two dimensions are independent. If damaging structure A removes aspect X but leaves Y intact, and damaging structure B removes Y but leaves X intact, then X and Y are independent - each can be eliminated without the other. This bidirectional pattern is called a double dissociation - the gold standard of evidence in clinical neuropsychology, because it rules out the possibility that one aspect is just easier to disrupt than the other. The classic example is wanting versus liking: depleting dopamine eliminates wanting but not liking; disrupting opioid signaling reduces liking but not wanting. Two structures, two aspects, four conditions, separable both ways. Where only one direction of the dissociation has been demonstrated (damage to A removes X but no complementary case removes Y while sparing X), this chapter calls it a single dissociation and notes the gap. A single dissociation is evidence of separability but not proof of full independence - the missing direction could reflect a lack of relevant patient cases rather than a genuine asymmetry. This chapter states which type of dissociation each dimension has earned.
Tool 2: the Atomicity Test. This test answers whether a candidate dimension is genuinely irreducible - whether it stands on its own rather than being a combination of others. It has three sub-tests, all of which must pass: non-composability (the dimension cannot be expressed as a combination of dimensions already in the set); independent variability (the dimension can change while every other dimension is held constant, demonstrated experimentally rather than by argument); and dedicated hardware (at least some neural substrate from Chapter 3’s inventory serves this dimension and not any other). A claim that, for instance, “alertness” is a separate dimension survives this test only if alertness has its own neural producer (the brainstem reticular activating system, a network of brainstem nuclei that gates whether the cortex is online at all), can be moved up or down independently of mood and attention, and cannot be reconstructed from a combination of other dimensions. Every dimension named in this chapter is run through the Atomicity Test; those that pass are retained, those that fail are reclassified as patterns (see Tool 4).
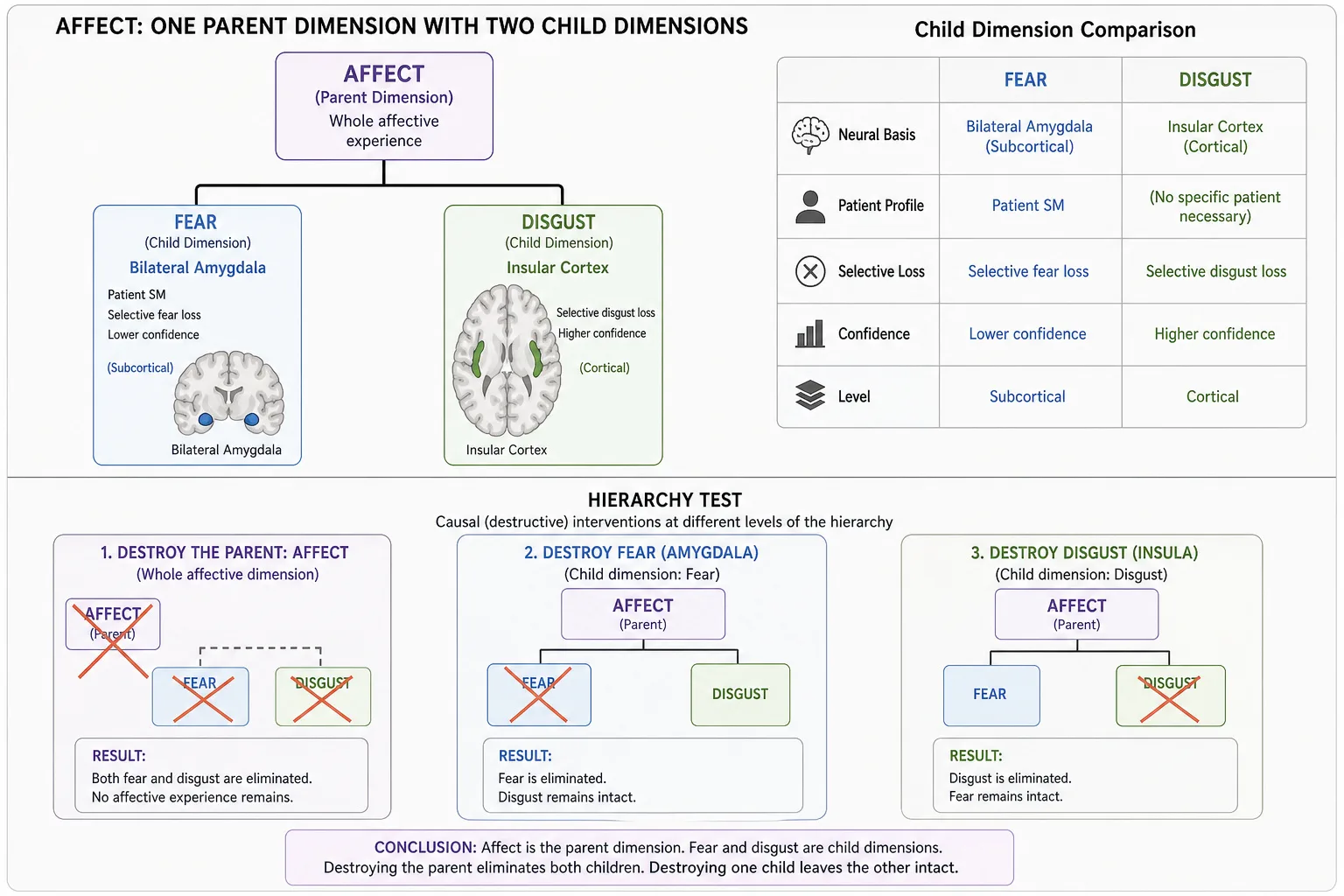
Tool 3: the Hierarchy Test. This test answers whether a fine-grained dimension nests inside a coarser one. Dimension B is a child of dimension A if eliminating A’s neural substrate also eliminates B, but eliminating B’s substrate leaves A intact. Color vision is a child of vision because destroying primary visual cortex (V1) eliminates color along with everything else visual, but destroying V4 - the cortical area specialized for color - leaves the rest of vision intact. Color and motion are siblings under vision, not separate dimensions of their own at the coarsest resolution. This test organizes the three resolution levels: Resolution Level 1 contains the parents, Resolution Levels 2 and 3 contain the children that nest within them.
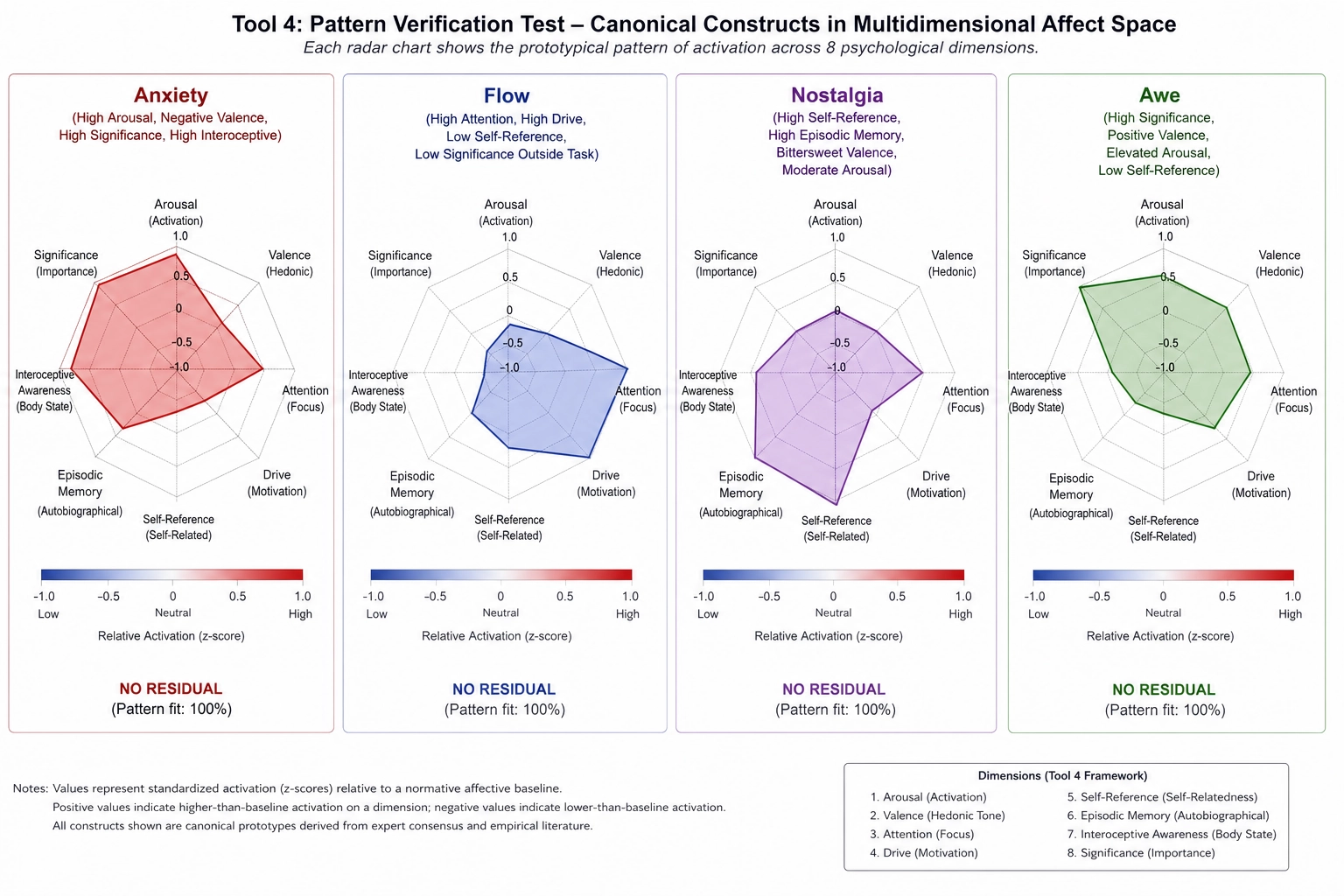
Tool 4: the Pattern Verification Test. This test answers what to do with named psychological states like anxiety, flow, nostalgia, and awe. These are real, named, frequently invoked. They are also not dimensions. The test maps the construct onto specific values across existing dimensions, then checks whether altering any single component dimension shifts the experience out of the named state. If anxiety can be turned into something other than anxiety by reducing arousal alone (a beta-blocker) without changing anything else about the experience, anxiety is a pattern across dimensions, not a dimension. The test treats psychology’s century of named states as regions in dimension space - recoverable from the dimensions, not additional to them.
| Tool | Question it answers | Evidence required | Pass criteria |
|---|---|---|---|
| Tool 1: Dissociation Test | Are two dimensions independent? | Damage to structure A removes X but not Y; damage to structure B removes Y but not X (double dissociation). Single dissociation accepted with noted gap. | Both directions demonstrated for full independence; one direction for separability |
| Tool 2: Atomicity Test | Is this dimension irreducible? | Non-composability (not a sum of others), independent variability (experimentally demonstrated), dedicated hardware (from Ch3 inventory) | All three sub-tests pass |
| Tool 3: Hierarchy Test | Does dimension B nest inside dimension A? | Eliminating A’s substrate also eliminates B; eliminating B’s substrate leaves A intact | Asymmetric elimination pattern |
| Tool 4: Pattern Verification Test | Is this psychological construct a dimension or a pattern? | Map construct to dimension values; perturb each component; check for residual | Construct decomposes fully into existing dimensions with no residual |
A note on evidence quality. Chapter 2 assigned each dimension an evidence rating - Strong, Moderate, or Preliminary - and those ratings are reused verbatim here, not re-derived. Strong means multiple independent lesion or dissociation studies, replicated across decades and patient populations. Moderate means consistent evidence from a smaller number of studies, sometimes resting on a single well-characterized patient. Preliminary means suggestive evidence that has not yet accumulated to the level of consensus.
A note on confidence tiers. Chapter 3 established that the brain’s hardware divides into two broad tiers for Khozai’s purposes: higher confidence systems whose activity is cortical and therefore readable by brain encoding models like TRIBE v2, and lower confidence systems whose activity is subcortical and therefore not directly predictable from cortical-only models. Every dimension in this chapter inherits a confidence tier from the hardware that produces it. Dimensions driven by cortical structures (vision, audition, face recognition, language, social cognition) sit at higher confidence. Dimensions driven by subcortical structures (arousal, fear, hedonic response) sit at lower confidence. Some dimensions span both tiers - their cortical effects are readable but their subcortical drivers are not. The chapter states the tier for each dimension.
A note on naming. The dimension named Interoceptive in this chapter is the experiential dimension - the awareness of internal body state. The receptor system that contributes to it is named visceral afferents in Chapter 2’s Premise 2 - the sensory nerves carrying information from internal organs to the brain. Both terms are correct; they refer to different things. This chapter uses Interoceptive consistently for the dimension and does not silently swap them.
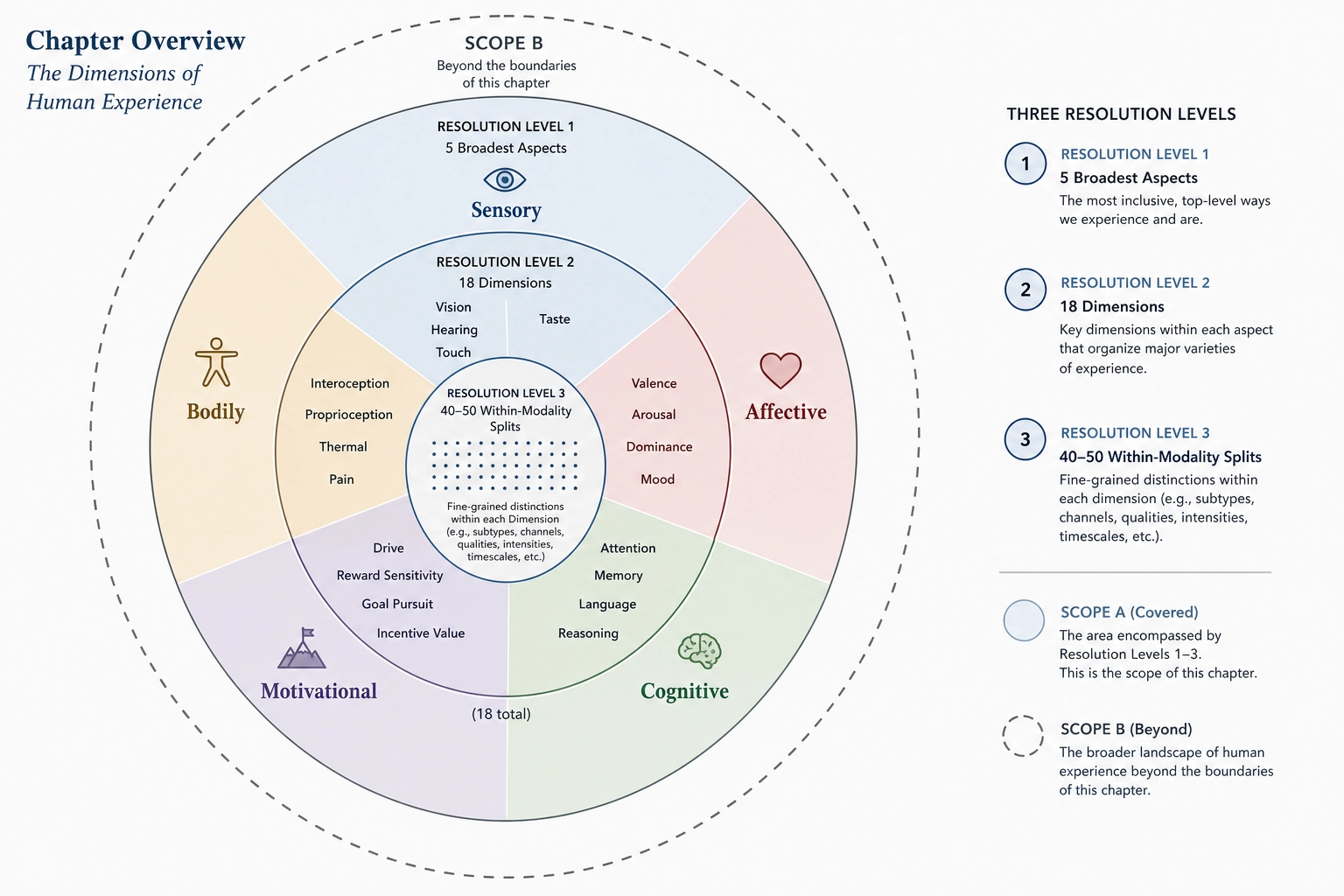
The chapter proceeds outward from the coarsest decomposition. 2. walks through the five dimensions of Resolution Level 1. 3. expands the sensory dimension into ten modalities and adds eight non-sensory dimensions to reach the eighteen of Resolution Level 2. 4. cuts deeper into specific modalities - color, motion, face recognition, music, episodic memory, fear - to reach the within-modality splits of Resolution Level 3 (seventeen enumerated sub-dimensions in v1, with the set open to growth as new dissociations are discovered). 5. applies the Pattern Verification Test (Tool 4) to four named psychological constructs: anxiety, flow, nostalgia, awe. 6. ends with the spanning question, which is falsifiable but never provable.
2. Resolution Level 1: The Five Broadest Aspects
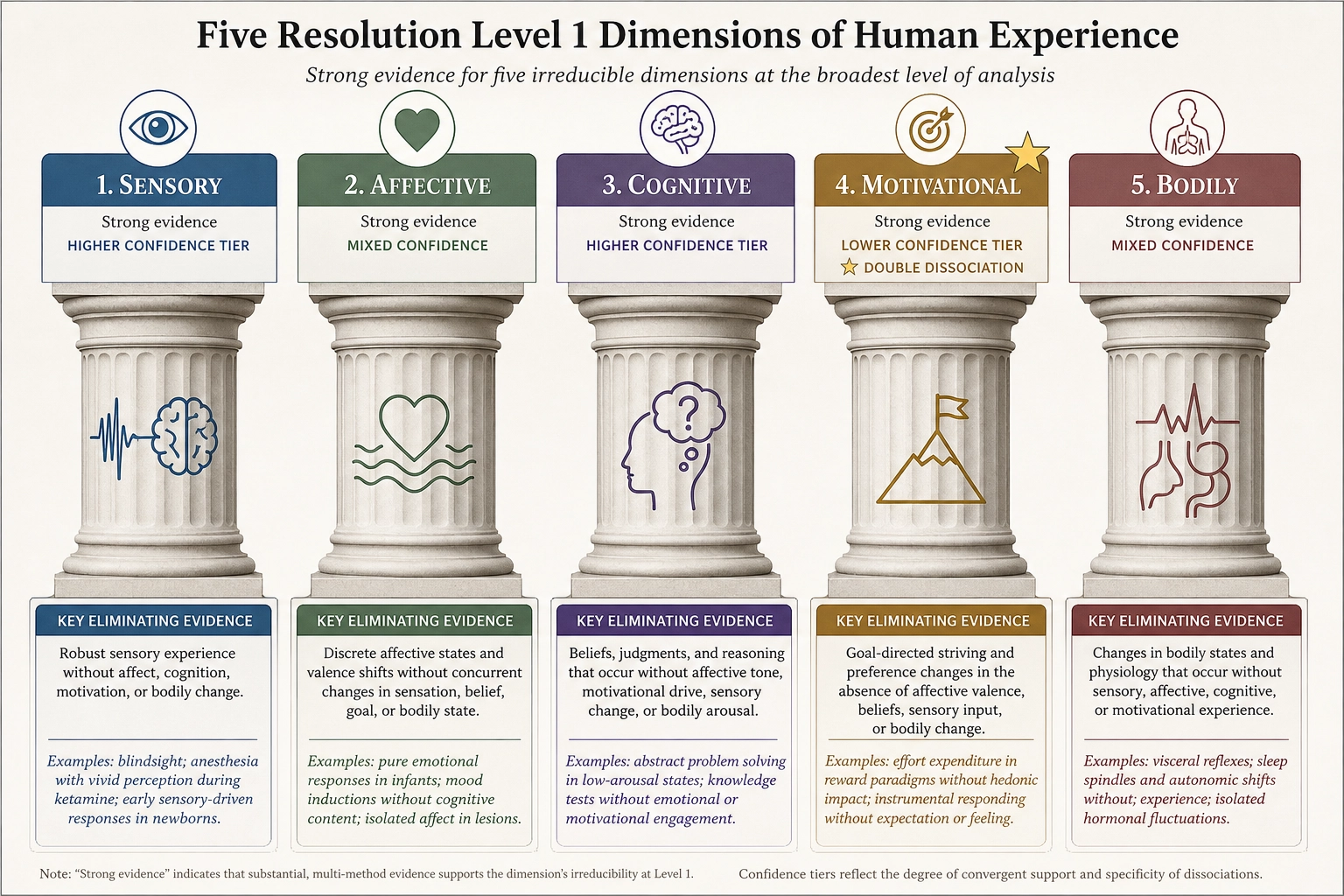
At the coarsest resolution, human experience separates into five aspects. Each survives as an aspect of experience even when the others are catastrophically reduced. Each can be eliminated by damage to specific neural structures while the others remain intact. This is the level at which the question “what is happening to this person right now?” can be answered by a small number of independent factors, before any further specification.
In the vector architecture from Chapter 2, these five aspects are the broadest axes of Ve - the experiential state vector. Each axis is a dimension along which a viewer’s experience can vary independently. The eighteen dimensions of Resolution Level 2 (3.) refine these five into a more granular coordinate system for the same space.
| Dimension | Eliminating evidence | Dissociation type (Tool 1) | Key dissociation partner | Evidence rating | Confidence tier | Classification (Tool 5) |
|---|---|---|---|---|---|---|
| Sensory | Bilateral cortical destruction (V1, A1) | Single - each modality dissociates from others, but no single lesion removes all sensation while sparing everything else | Affective (SM: fear gone, senses intact) | Strong | Higher (cortical) | State producer |
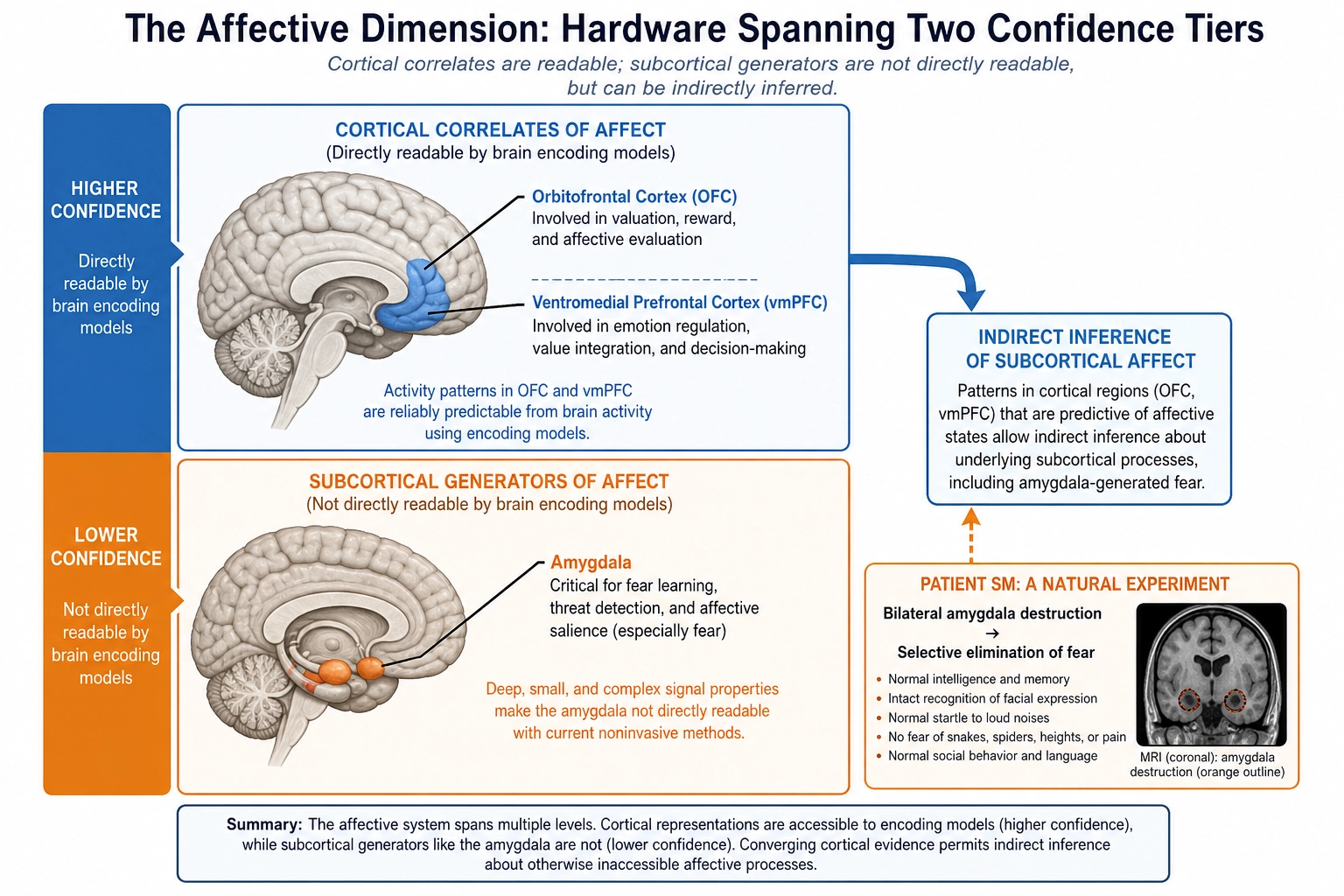
| Affective | Bilateral amygdala (SM), orbitofrontal damage | Single at RL1 level; double at RL2 (wanting/liking) | Sensory (cortical blindness: senses gone, affect intact) | Strong | Mixed - amygdala lower, OFC higher | State producer |
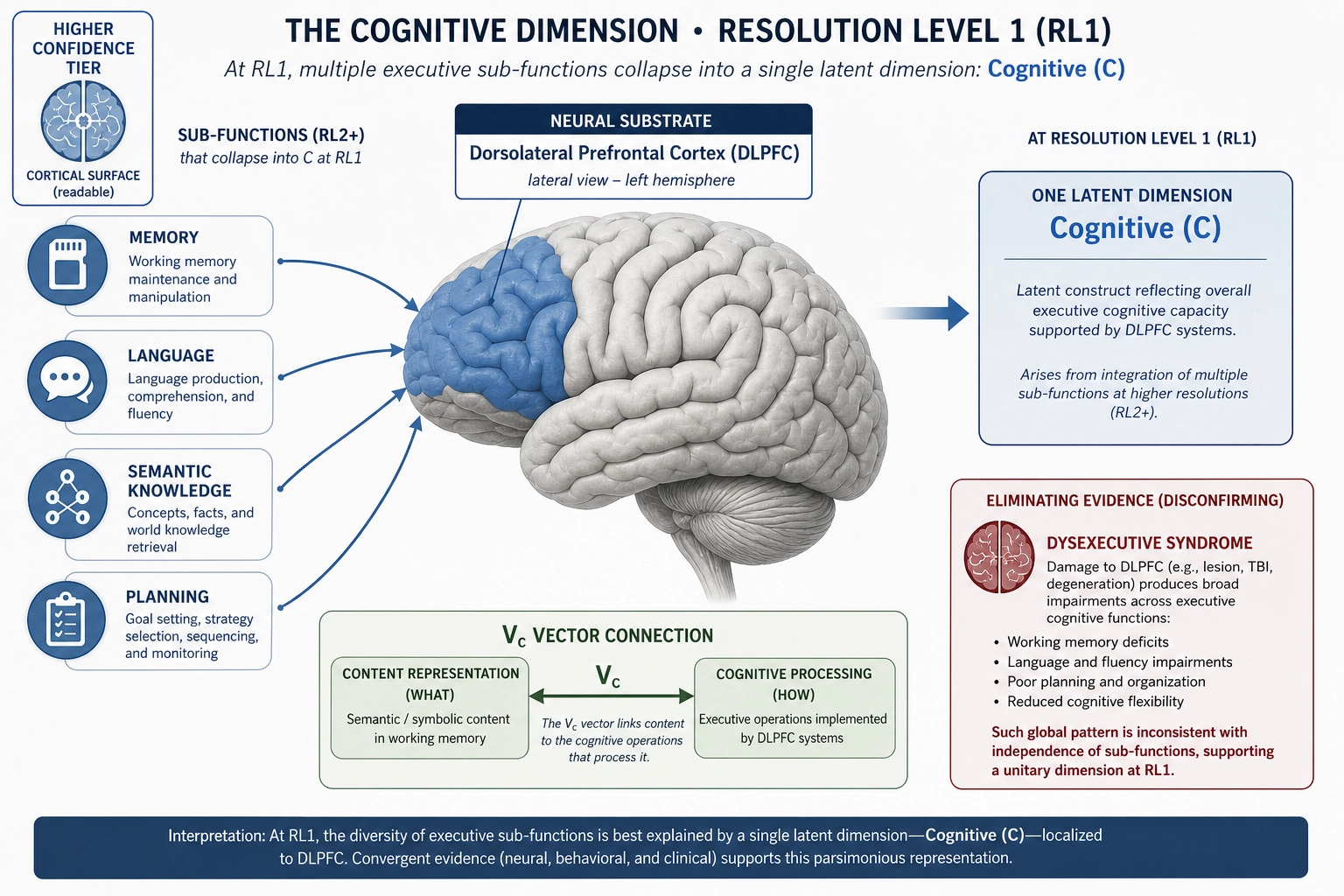
| Cognitive | Dorsolateral prefrontal damage (dysexecutive syndrome) | Single - cognition removed with others intact; no clean case of others removed with cognition specifically preserved | Affective (SM: affect disrupted, cognition intact) | Strong | Higher (cortical) | State producer |
| Motivational | Dopamine depletion (mesolimbic pathway) | Double - dopamine depletion removes wanting but not liking; opioid antagonists remove liking but not wanting | Affective/Hedonic [3] | Strong | Lower (subcortical - VTA/ventral striatum) | State producer |
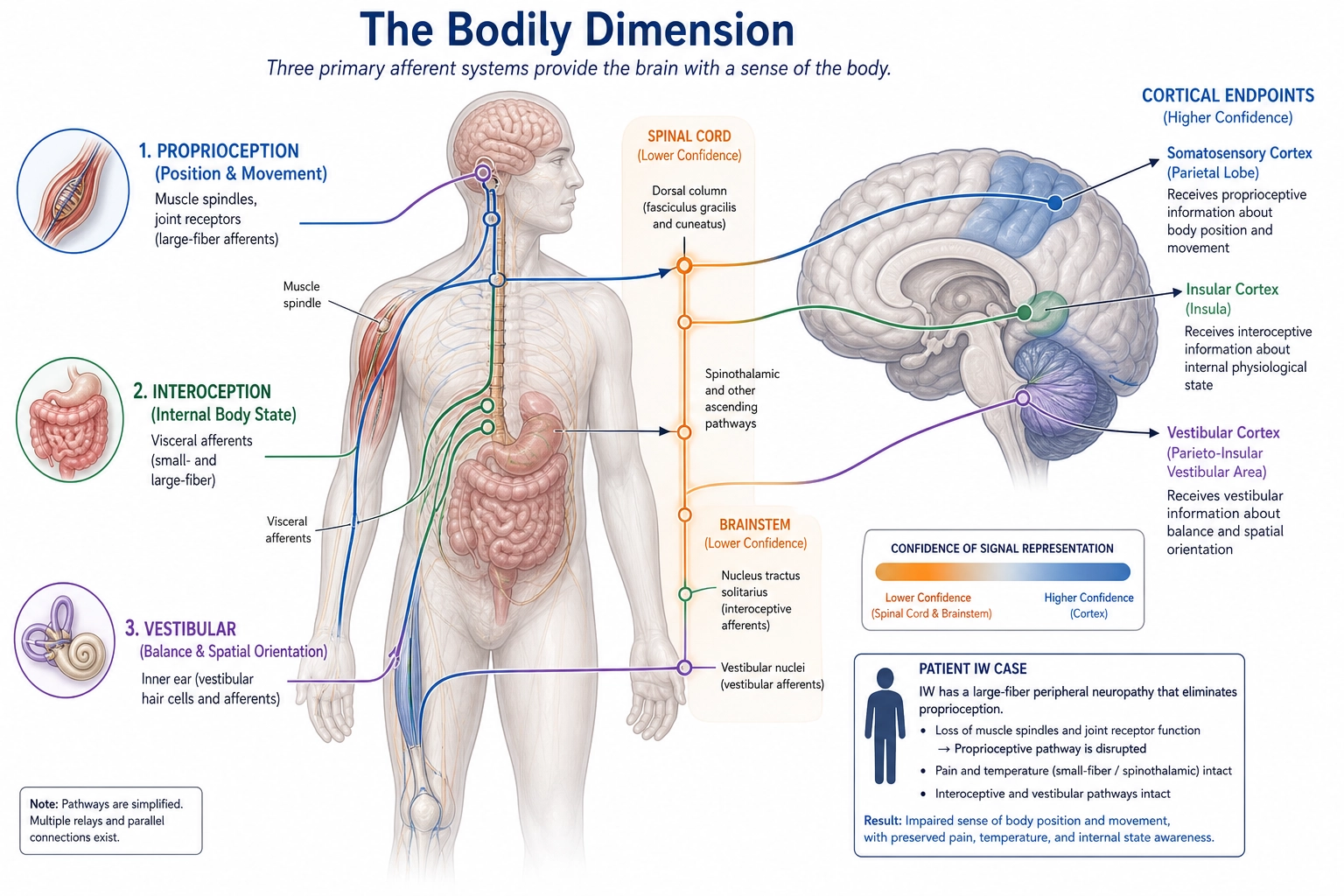
| Bodily | Spinal cord transection, large-fiber neuropathy (patient IW) | Single - body sense removed with others intact; no clean complementary case | Sensory-above-lesion (spinal patients: body sense gone, vision/hearing intact) | Strong | Mixed - spinal/brainstem lower, insular cortex higher | State producer |
Sensory
The Sensory dimension covers all of what reaches the experiencing mind through the ten receptor systems cataloged in Chapter 3 - what is seen, heard, felt, smelled, tasted, sensed in the body, sensed in the orientation of the body in space. At this resolution, it is one dimension. It splits into ten in 3..
The eliminating evidence is cortical destruction of individual sensory areas. Bilateral destruction of primary visual cortex (V1) produces cortical blindness - the patient is awake, alert, and capable of emotion, thought, motivation, and bodily feeling, but reports no visual experience. Bilateral destruction of primary auditory cortex produces cortical deafness with the same pattern in the auditory channel. No single case in the literature demonstrates simultaneous loss of all ten sensory modalities with perfect preservation of everything else - such a case would require bilateral destruction of every primary sensory cortex while sparing prefrontal, limbic, and subcortical structures, a pattern that natural lesions and surgical cases have not produced. The evidence for Sensory as a dimension therefore rests on convergence: each individual modality can be selectively eliminated (shown in 3.), and every elimination case preserves the non-sensory dimensions. The convergence is Strong; the single-case demonstration is absent.
Dissociation status (Tool 1). Single dissociation at the RL1 level. Each sensory modality dissociates cleanly from non-sensory dimensions (patient SM lost fear but retained all senses; dysexecutive patients lost planning but retained all senses). The reverse direction - all senses gone, everything else intact - is supported by convergence across modality-specific cases but not by a single multi-modal elimination case.
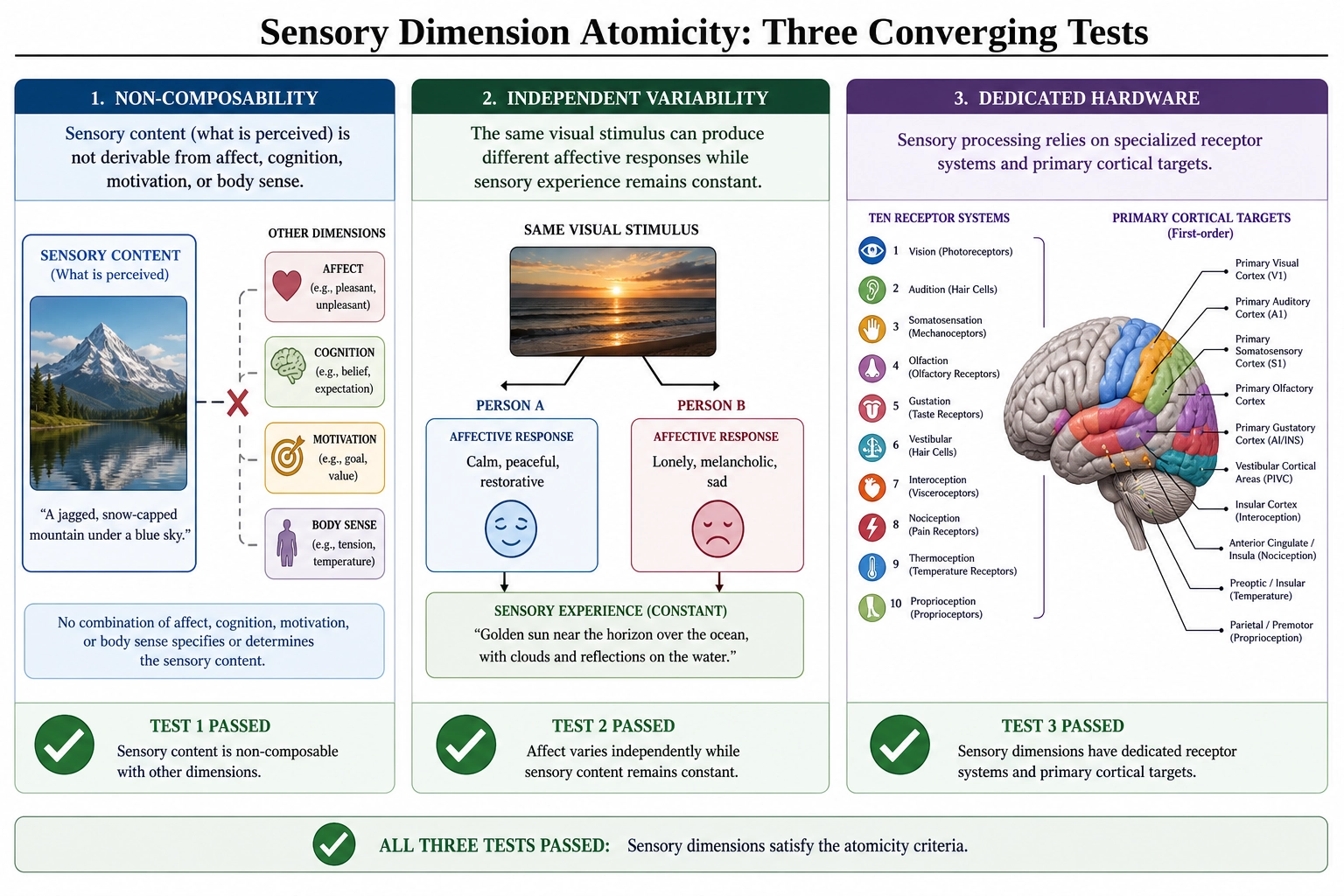
Atomicity check (Tool 2). Non-composability: Sensory is not a sum of Affective, Cognitive, Motivational, or Bodily - it carries content (what is perceived) that none of the others provide. Independent variability: sensory experience varies independently of affect (identical visual stimulus can produce different affective responses), cognition (perception without recognition in agnosia), motivation (perception without wanting), and body sense (vision intact after spinal transection). Dedicated hardware: the ten receptor systems and their primary cortical targets (Chapter 3 1.) serve Sensory and not the other dimensions. Passes all three sub-tests.
Khozai implication. The Sensory dimension is the entry point for all screen-mediated content. V0 (the physical stimulus vector) measures what the receptor systems will receive; the Sensory axis of Ve measures the experiential result. Cortical sensory areas sit at higher confidence - TRIBE v2 can predict visual and auditory cortical activation from content features. The framework can therefore estimate Sensory engagement with reasonable confidence. The practical consequence: when the framework attributes a behavioral outcome to “strong visual engagement,” it would be referencing activation in cortical areas that the encoding model can read, not subcortical processing it cannot.
Affective
The Affective dimension covers emotion in its broadest form - the valenced, often arousing aspect of experience that gives stimuli their pleasantness or unpleasantness, their threat or safety, their pull or push.
The eliminating evidence comes most cleanly from patient SM, a woman with bilateral amygdala destruction caused by Urbach-Wiethe disease, a rare genetic disorder that produces calcification of specific medial temporal structures (the neuroscientist Ralph Adolphs and colleagues [1], J. Neurosci. 15(9):5879-5891; Feinstein et al. [15]; ongoing case series across two decades). SM has intact vision, hearing, language, memory, and social reasoning. What she does not have is fear. She does not show fear responses to snakes, spiders, threatening films, or haunted attractions. Other case studies and large patient series of frontal and limbic damage extend this to the broader affective dimension: severe orbitofrontal damage can blunt valenced response across emotions while sparing perception and cognition. The evidence is Strong.
Dissociation status (Tool 1). Single dissociation at the RL1 level. Affect can be selectively reduced (SM, orbitofrontal patients) while Sensory, Cognitive, Motivational, and Bodily remain intact. The complementary direction - all non-affective dimensions reduced while affect remains - is not demonstrated by a single case, though cortical-blind patients retain affective responses to non-visual stimuli, and dysexecutive patients retain emotion. At Resolution Level 2, the Motivational dimension provides a full double dissociation via the wanting-liking split (see 2. Motivational below). At RL1, the dissociation is single.
Atomicity check (Tool 2). Non-composability: Affective valence (pleasant/unpleasant) is not derivable from Sensory intensity, Cognitive appraisal, or Motivational drive alone - the same sensory input can produce opposite valences in different contexts. Independent variability: pharmacological manipulation of serotonin (SSRIs) shifts affective valence without altering sensory acuity, cognitive performance, or body sense. Dedicated hardware: amygdala, orbitofrontal cortex, and ventromedial prefrontal cortex serve affective processing as their primary function (Chapter 3 2.-3.). Passes all three sub-tests.
Khozai implication. The Affective dimension is the experiential axis most directly relevant to content impact - whether a viewer finds content pleasant, aversive, moving, or flat. Its hardware spans both tiers: the amygdala is subcortical (lower confidence - TRIBE v2 cannot directly predict amygdala activation), but the orbitofrontal and ventromedial prefrontal cortex are cortical (higher confidence). The framework is designed to estimate the cortical component of affective response but has a blind spot for the subcortical component, particularly for fear and threat processing. When the framework reports “strong affective engagement,” it is primarily reading the cortical signature; the subcortical contribution is inferred from cortical correlates, not directly measured. This asymmetry is stated, not hidden.
Cognitive
The Cognitive dimension covers what the experiencing mind is doing with what it perceives - recognizing, categorizing, planning, sequencing, predicting, reasoning, holding things in mind.
The eliminating evidence comes from severe prefrontal damage producing dysexecutive syndrome - a pattern of disrupted planning, sequencing, abstraction, and goal-directed behavior documented across hundreds of clinical case series since the early lesion literature (the neuropsychologist Alexander Luria (1966) [19]; the neuropsychologist Tim Shallice (1982) [28]; Stuss and Benson (1986) [29]). Patients with severe dorsolateral prefrontal damage retain perception, emotion, basic motivation, and bodily feeling, but cannot organize behavior toward goals, hold complex sequences in mind, or solve problems requiring multiple steps. The evidence is Strong.
Within the Cognitive dimension, more specific aspects (memory, language, semantic knowledge, planning) are separable from each other at finer resolution - patient HM (the neurosurgeon William Scoville and the neuropsychologist Brenda Milner [26]) lost the ability to form new long-term memories after bilateral medial temporal lobe surgery while retaining language, intelligence, and short-term thought, demonstrating that memory formation is itself a separable component (treated in 4.). At Resolution Level 1, all of these collapse into a single Cognitive aspect that can be reduced as a whole while Sensory, Affective, Motivational, and Bodily aspects remain functional.
Dissociation status (Tool 1). Single dissociation. Cognition can be selectively reduced (dysexecutive syndrome) while Sensory, Affective, Motivational, and Bodily remain intact. The complementary direction - cognition preserved while all other dimensions are removed - is not demonstrated by a single case. However, patient SM (bilateral amygdala) shows intact cognition with disrupted affect, and cortical-blind patients show intact cognition with disrupted vision. These converging single dissociations from multiple partner dimensions provide strong evidence of independence even without a single double-dissociation case.
Atomicity check (Tool 2). Non-composability: Cognitive processing (recognizing, sequencing, predicting) is not reducible to a combination of Sensory input plus Affective response plus Motivational drive - agnosic patients perceive without recognizing, demonstrating that recognition is a separate operation. Independent variability: cognitive load can be increased (by task complexity) without changing sensory input, affective state, or body sense. Dedicated hardware: dorsolateral prefrontal cortex, lateral parietal cortex, and temporal association areas serve cognitive processing as their primary function (Chapter 3 2.). Passes all three sub-tests.
Khozai implication. Cognitive engagement is what permits a viewer to make sense of narrative, recognize references, understand intent, predict what comes next. Physical stimulus properties drive Sensory engagement directly; Cognitive engagement is mediated by recognition and interpretation - the same pixel values produce different cognitive engagement depending on whether the viewer recognizes what they depict. Cognitive hardware is predominantly cortical (dorsolateral prefrontal, lateral parietal, temporal association areas), placing this dimension at higher confidence for TRIBE v2 prediction. Vc (the content representation vector) approximates what cognitive processing the content is likely to elicit; the Cognitive axis of Ve represents the experiential result of that processing.
Motivational
The Motivational dimension covers wanting - the pull toward something, the drive to approach, the orientation of behavior toward a goal, separable from whether the goal feels good when reached.
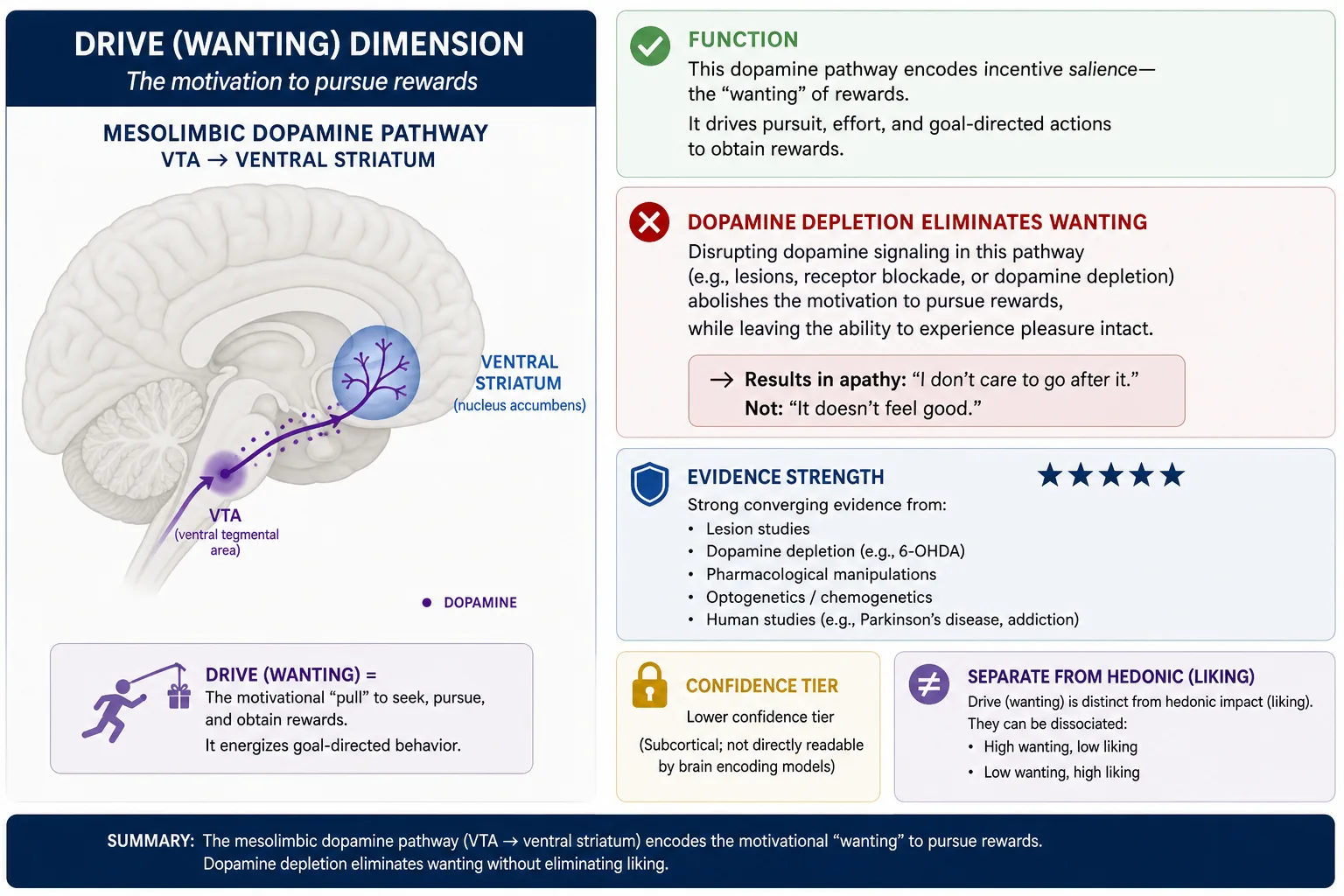
The eliminating evidence is dopamine depletion, established in the seminal review by the neuroscientists Kent Berridge and Terry Robinson [3] (Brain Research Reviews) and extended through three decades of subsequent work. Depleting dopamine in the mesolimbic pathway - the dopamine projection running from midbrain (ventral tegmental area) to ventral striatum that carries reward signals - eliminates wanting (the pursuit of a reward) while leaving liking (the hedonic response to actually receiving it) intact. Animals with dopamine-depleted reward systems still show normal facial reactions to sweet tastes (the liking response, mediated by opioid systems) but no longer work to obtain rewards (the wanting response, mediated by dopamine). The dissociation is double: opioid antagonists reduce liking without reducing wanting. A complication: the strongest evidence for this double dissociation comes from rodent models. Human evidence is consistent but less pharmacologically precise. The clearest human demonstration comes from Evans and colleagues [42] (2006), who used PET imaging in Parkinson’s disease patients and showed in Annals of Neurology that sensitized ventral striatal dopamine transmission correlated with compulsive drug-seeking behavior (wanting) but not with subjective pleasure ratings (liking). Berridge and Robinson [43] (2016) reviewed the broader human evidence in American Psychologist, confirming that the wanting-liking dissociation extends from rodent models to human addiction, Parkinson’s disease, and pharmacological challenge studies, though the pharmacological precision achievable in animal preparations has not been fully replicated in human studies. The framework treats the dissociation as established because the human clinical evidence converges with the animal evidence and no published counter-evidence exists, but the cross-species inference is noted. The evidence is Strong.
Dissociation status (Tool 1). Double dissociation - the only RL1 dimension that achieves this standard. Dopamine depletion removes wanting but not liking; opioid antagonists remove liking but not wanting. This is the textbook double dissociation in affective neuroscience (as established in Chapter 2 2..4 [3]). At RL1, this double dissociation separates Motivational from Affective. At RL2, it becomes the basis for splitting Motivational into Drive (wanting) and Hedonic (liking) as separate dimensions.
Atomicity check (Tool 2). Non-composability: wanting is not a combination of Sensory input plus positive Affect - dopamine-depleted animals experience both but want neither. Independent variability: dopamine agonists increase wanting without changing sensory acuity, cognitive performance, or body sense; caffeine increases alertness (Arousal) without necessarily increasing wanting. Dedicated hardware: the mesolimbic dopamine pathway (VTA to ventral striatum) serves wanting as its primary function, classified as a state producer in Chapter 3’s neurochemical inventory. Passes all three sub-tests.
Khozai implication. The Motivational dimension is what drives a viewer to keep watching, to seek out more of something, to follow through on a call to action. Its hardware is subcortical (VTA and ventral striatum), placing it at lower confidence for TRIBE v2 - the encoding model cannot directly predict mesolimbic dopamine activity from content features. The framework is designed to infer motivational engagement from its cortical correlates (prefrontal goal-representation activity, which is readable) and from Vp (behavioral signals like watch-through rate and return visits, which are directly measured). The dimension is real and important, but its direct neural signature sits in Khozai’s blind spot. Resolution Level 2 will split it into Drive and Hedonic on exactly the dopamine/opioid evidence.
Bodily
The Bodily dimension covers the experiential aspect of being in a body - proprioception (the sense of where one’s limbs are), interoception (the sense of internal body state), the felt sense of physical presence and embodiment.
The eliminating evidence comes from spinal cord transection - a complete spinal injury at high cervical level produces loss of body sensation below the lesion, with progressive eliminations of bodily aspects of experience the higher the lesion sits. Patients retain Sensory experience above the lesion (vision, hearing), affective response, cognitive function, and motivational drive. What changes is the felt sense of having a lower body. Patient IW (described by the neurologist Jonathan Cole (1995) [8] in Pride and a Daily Marathon) provides a more selective case: a sensory neuropathy that destroyed his large-fiber afferents below the neck, eliminating proprioception while leaving pain and temperature sensation intact. He retained motor capability but lost the automatic sense of where his limbs were in space, and had to consciously re-learn movement by visual guidance. The evidence is Strong.
Dissociation status (Tool 1). Single dissociation. Body sense can be selectively reduced (spinal transection, patient IW’s neuropathy) while Sensory (above lesion), Affective, Cognitive, and Motivational remain intact. The complementary direction - body sense preserved while all other dimensions are removed - is not demonstrated by a single case. However, cortical-blind patients retain body sense, dysexecutive patients retain body sense, and SM retains body sense, providing converging evidence from the partner-dimension side.
Atomicity check (Tool 2). Non-composability: body sense is not a sum of Sensory input plus Affective response - patient IW has intact vision and affect but no proprioception, demonstrating that body-position awareness is a separate experiential quality. Independent variability: proprioceptive signals can be experimentally perturbed (vibration illusions, galvanic vestibular stimulation) without changing visual input, affective state, or cognitive load. Dedicated hardware: the proprioceptive and interoceptive receptor systems (Chapter 3 1.) and the insular cortex (Chapter 3 2.) serve body-state monitoring as their primary function. Passes all three sub-tests.
Khozai implication. The Bodily dimension is the aspect of experience least directly engaged by video content viewed through screens. Most of what a video does is Sensory (visual and auditory), Cognitive, Affective, and Motivational; its Bodily engagement is indirect, mediated by the brain’s predictive processing rather than by direct receptor stimulation. The hardware spans both confidence tiers: the insular cortex’s body-state representation is cortical (higher confidence, readable by TRIBE v2), but the spinal and brainstem pathways that feed it are subcortical (lower confidence). Chapter 3 4. traced the body-state monitoring pathway and noted this confidence transition. The framework includes Bodily as a dimension because excluding it would leave the dimension set incomplete - there are content forms (immersive virtual reality, exercise content, autonomous sensory meridian response material) that engage Bodily aspects more directly - and because acknowledging Bodily as a separate dimension prevents accidentally reading bodily-feeling self-reports as affective ones.
These five dimensions exhaust Resolution Level 1. Every example reviewed selectively eliminates one while the others remain. Each is graded - partial damage produces partial reduction. Each is bounded - none can go negative, and each has a maximum determined by how strongly its hardware can be driven. Of the five, only Motivational achieves a full double dissociation (Tool 1); the other four rest on single dissociations supported by convergent evidence from multiple partner dimensions. All five pass the Atomicity Test (Tool 2). The next resolution refines each one further.
3. Resolution Level 2: Eighteen Dimensions
At finer resolution, the Sensory dimension splits into ten modalities - each one with selective evidence that it can be eliminated independently of the other nine - and the remaining four Resolution Level 1 aspects expand to expose eight further independent dimensions in Affect, Motivation, and Cognition. Eighteen dimensions in total. Each is supported by its own elimination evidence.
Mapping to the vector architecture. The eighteen dimensions of Resolution Level 2 are the axes of Ve as defined in Chapter 2. Chapter 2 4..5 gave Ve an initial operating set of five dimensions (valence, arousal, dominance, novelty, engagement) and flagged the list as incomplete. This chapter replaces that placeholder. The five RL1 dimensions map onto Ve’s initial set approximately: Affective covers valence, Motivational covers drive-related engagement, Cognitive covers dominance and novelty appraisal, and the Sensory and Bodily dimensions were absent from the initial set. The eighteen RL2 dimensions provide the full coordinate system: every point in Ve is now a position along eighteen named axes, each with its own elimination evidence and confidence tier. When later chapters reference “Ve predicts outcome X,” the prediction decomposes into specific values along these eighteen dimensions.
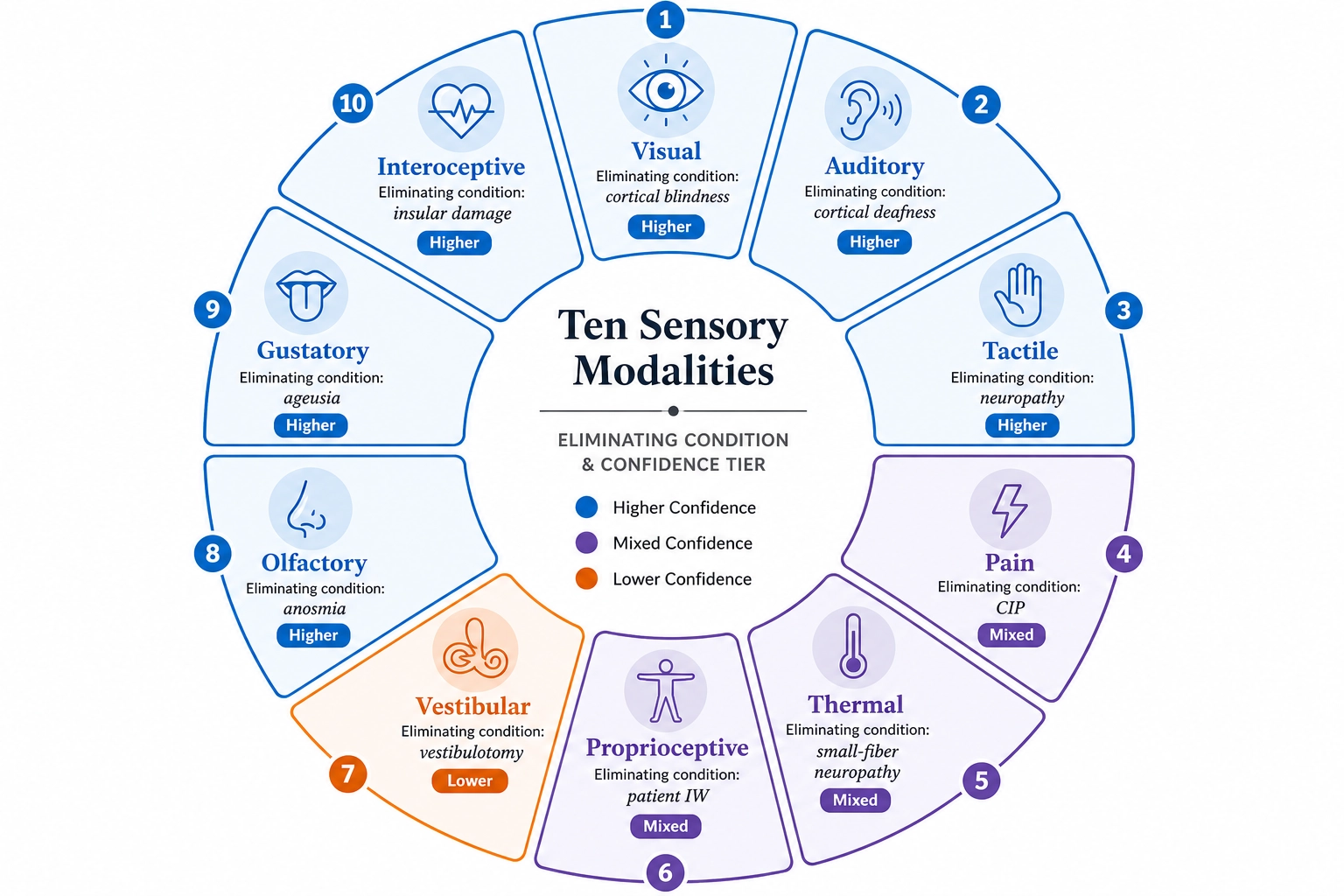
The Ten Sensory Modalities
| Modality | Eliminating lesion/condition | Key patient or study | Evidence rating | Confidence tier | Khozai engagement |
|---|---|---|---|---|---|
| Visual | Bilateral V1 destruction | Cortical blindness case series | Strong | Higher (cortical) | Primary - direct input channel |
| Auditory | Bilateral A1 destruction | Cortical deafness case series | Strong | Higher (cortical) | Primary - direct input channel |
| Tactile | Large-fiber neuropathy | Selective touch loss cases | Strong | Higher (cortical) | Absent in screen content |
| Pain | SCN9A mutation (CIP) | Congenital insensitivity patients | Strong | Mixed - nociceptors lower, ACC higher | Indirect - graphic content |
| Thermal | Small-fiber neuropathy | Selective temperature loss cases | Moderate | Mixed - thermoreceptors lower, insula higher | Indirect - predictive processing |
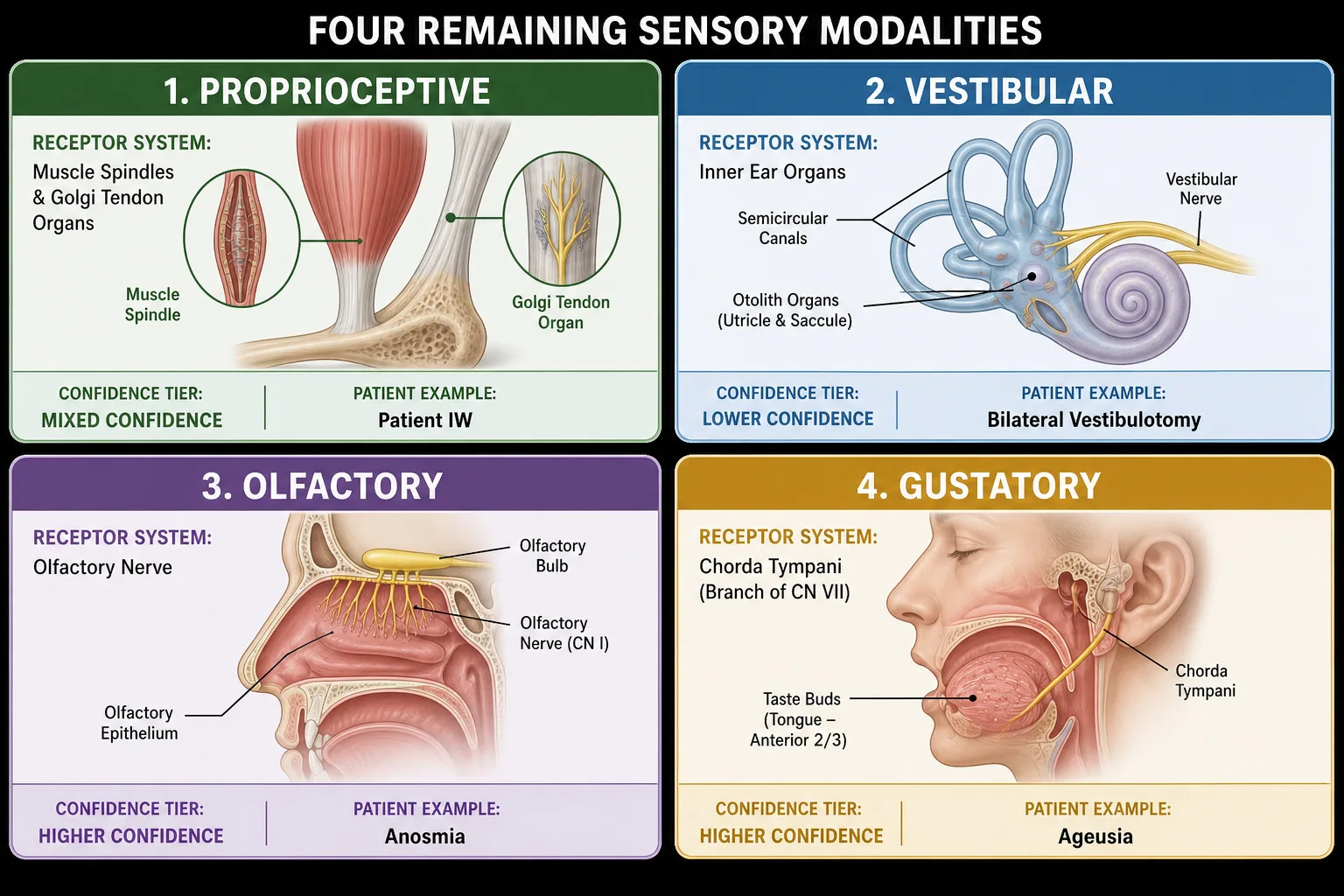
| Proprioceptive | Large-fiber neuropathy | Patient IW [8] | Strong | Mixed - spinal lower, somatosensory higher | Indirect - mirror system |
| Vestibular | Bilateral vestibulotomy | Post-Meniere’s surgical cases | Strong | Lower (peripheral organ) | Indirect - vection in immersive content |
| Olfactory | Olfactory nerve damage | Anosmia from head trauma | Strong | Higher (olfactory cortex) | Absent in screen content |
| Gustatory | Chorda tympani damage | Ageusia case series | Strong | Higher (gustatory cortex) | Absent in screen content |
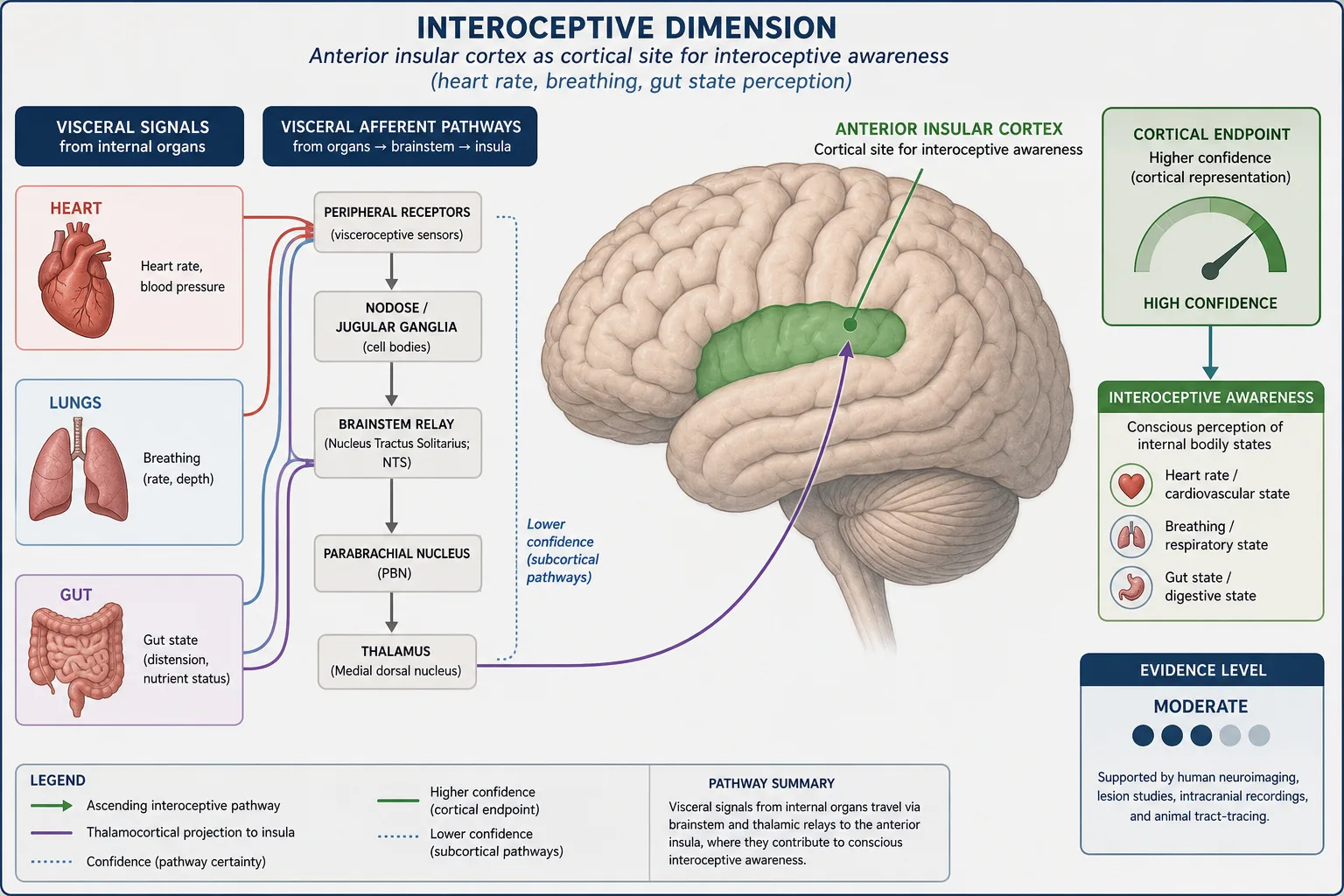
| Interoceptive | Anterior insular cortex lesion | [10]; insular lesion cases | Moderate | Higher (insular cortex) | Indirect - visceral responses to content |
Visual
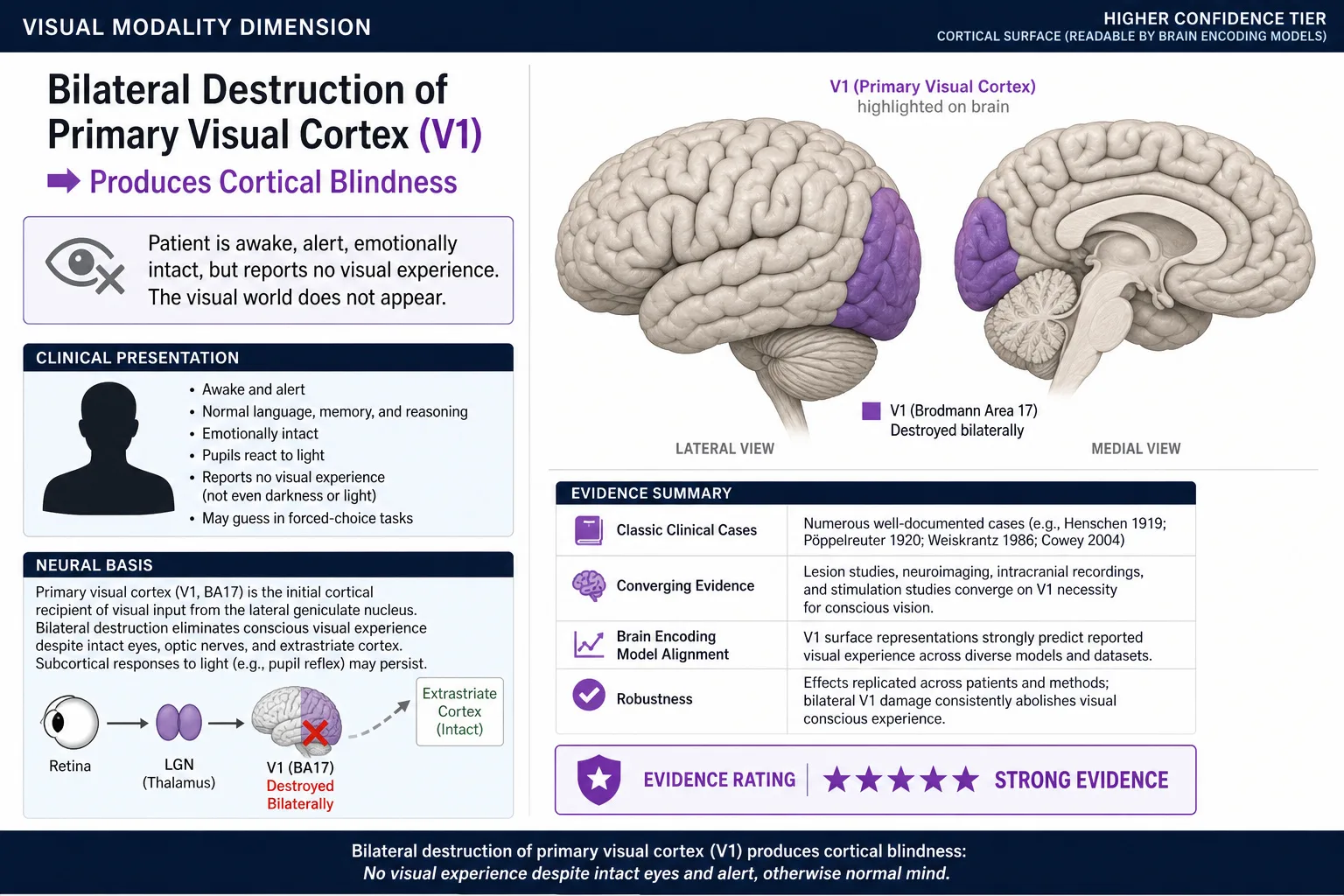
The eliminating evidence is cortical blindness - bilateral destruction of primary visual cortex (V1) produces a complete loss of visual experience while hearing, touch, taste, smell, body sense, and all non-sensory dimensions remain intact. The mechanism is direct: V1 receives the visual signal from the lateral geniculate nucleus (the thalamic relay for vision) and is the obligatory cortical entry point for visual processing. When it is destroyed bilaterally, no further visual cortical processing can occur. Cases include stroke patients, World War I and II soldiers with bilateral occipital injury, and surgical case studies. The evidence is Strong. Confidence tier: higher (cortical surface - V1 and downstream visual areas are directly readable by TRIBE v2).
Khozai implication. Visual is one of the two primary input channels for screen-mediated content. V0 measures the physical properties (luminance, color, motion, spatial frequency) that the visual receptor system will receive; the Visual axis of Ve measures the experiential result. Because visual cortex sits at higher confidence, TRIBE v2 can predict visual cortical activation from content features. This is the dimension where the framework’s measurement is strongest.
Auditory
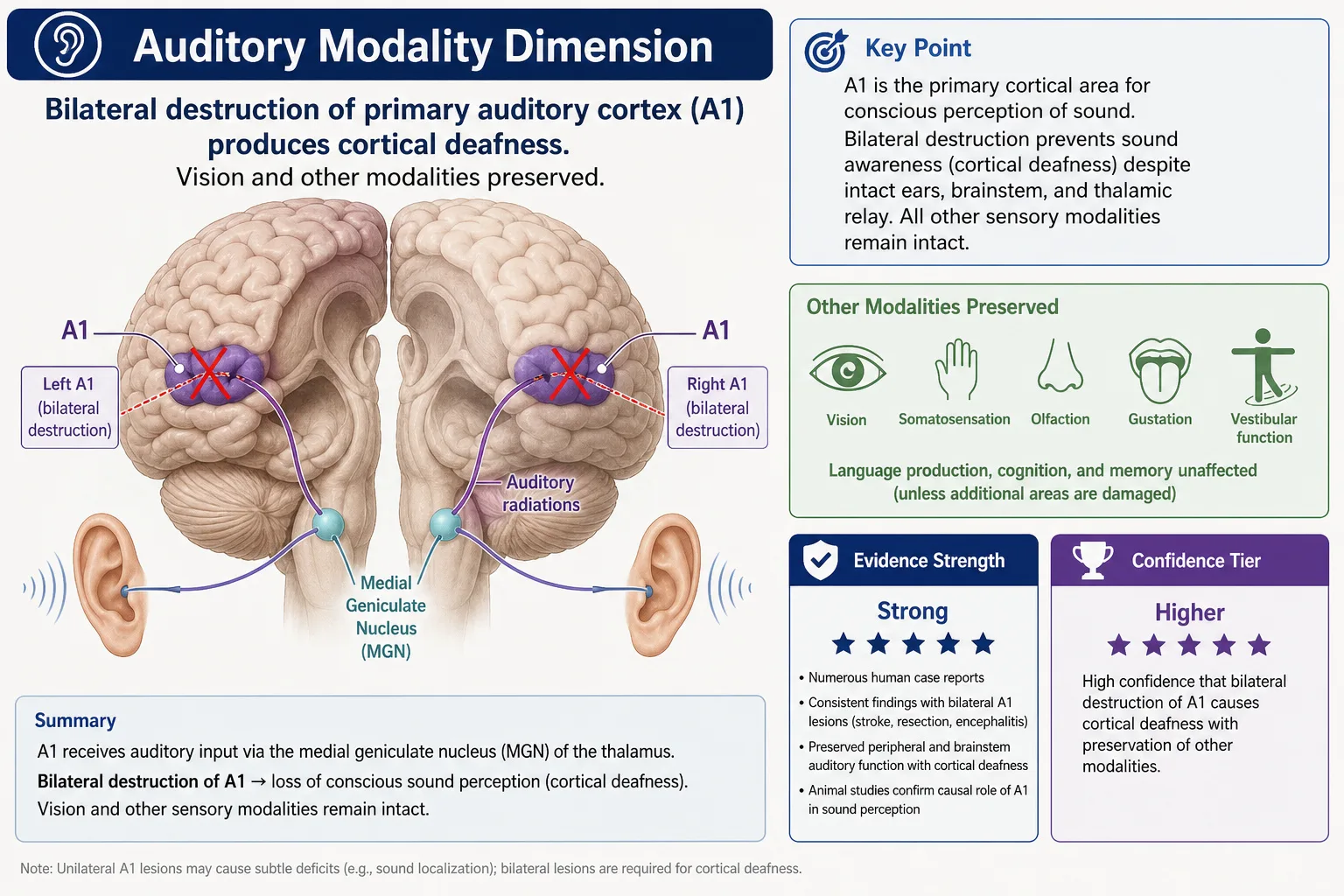
The eliminating evidence is cortical deafness - bilateral destruction of primary auditory cortex (A1) produces loss of auditory experience with vision and other modalities preserved. As with vision, the mechanism is direct: the medial geniculate nucleus (the thalamic relay for audition) projects to A1, and bilateral A1 destruction removes the obligatory cortical entry point for hearing. The evidence is Strong. Confidence tier: higher (cortical surface).
Khozai implication. Auditory is the second primary input channel for video content. The independence of Visual and Auditory justifies measuring audio properties (waveform, spectral content, temporal energy) on a separate Ve axis from visual properties - a content piece can be visually strong and auditorily weak, or vice versa. Both dimensions sit at higher confidence.
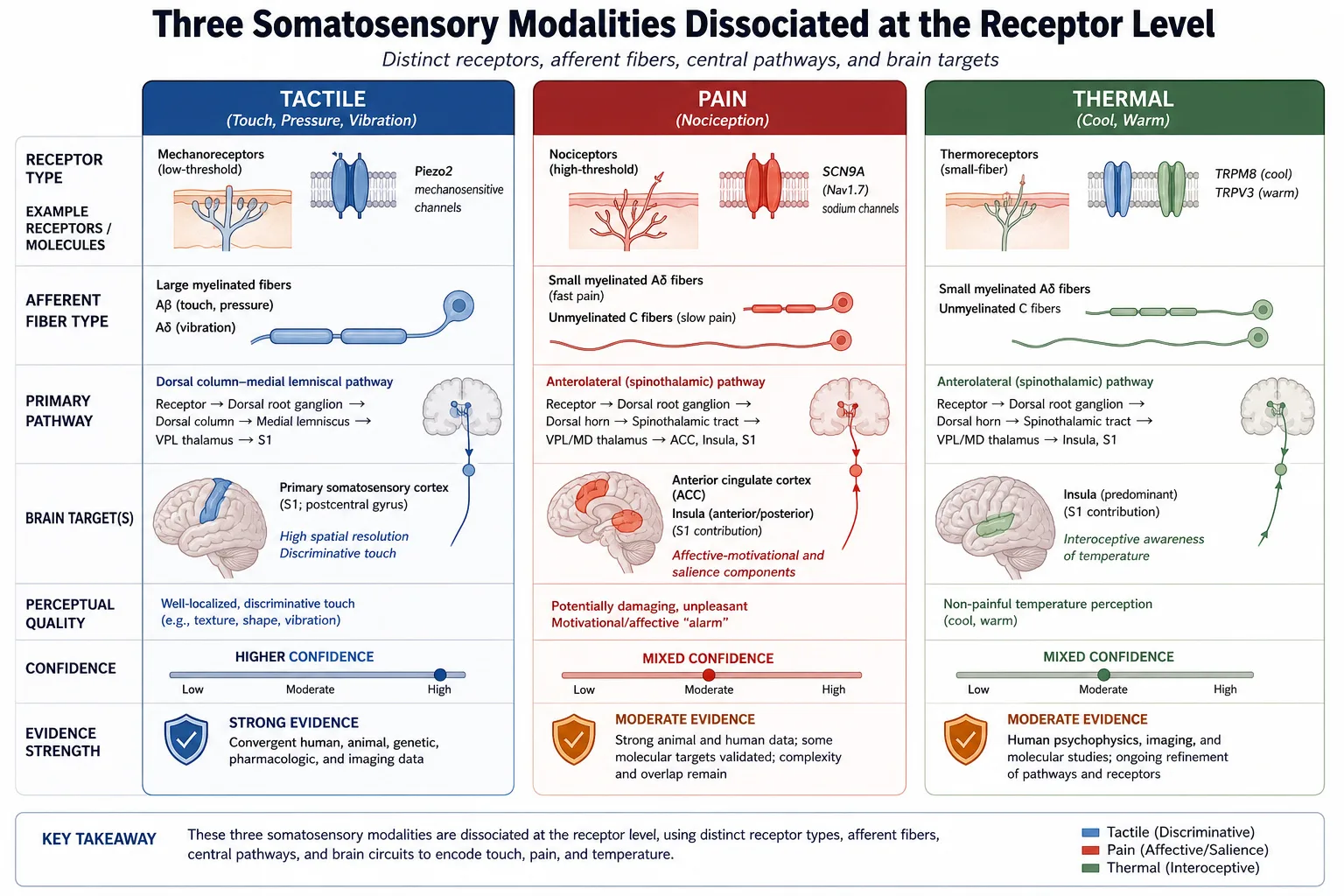
Tactile
The eliminating evidence is large-fiber neuropathy that selectively eliminates touch - fine discrimination of mechanical pressure, texture, and vibration - while leaving pain and temperature sensation intact (because pain and temperature travel on different, smaller-diameter fibers). Selective tactile loss separates touch from pain at the receptor level: the two travel separate pathways from skin to brain and reach distinct cortical processing areas (somatosensory cortex for touch, anterior cingulate and insula for pain). The evidence is Strong. Confidence tier: higher (somatosensory cortex is cortical surface).
Khozai implication. Tactile engagement is absent from screen-mediated video content, but the dimension is included because the framework’s claim to span Experience Space requires that it not exclude sensory channels based on the current measurement context. The dimension set is defined by neurology, not by what screens can deliver.
Pain
The eliminating evidence is congenital insensitivity to pain (CIP) - a condition caused by mutations in the SCN9A gene (encoding the Nav1.7 sodium channel) that produces nociceptors (pain receptors) that cannot transduce tissue-damage signals. Affected individuals have intact touch, temperature, proprioception, and all other modalities but report no pain experience even from severe injury. The selective elimination is genetic and lifelong. The evidence is Strong. Confidence tier: mixed - nociceptors and spinal processing at lower confidence, but the cortical pain signature (anterior cingulate cortex, insula) sits at higher confidence.
Khozai implication. Pain is a separate dimension from Tactile and Affective, even though it has affective character. Content that triggers pain responses (graphic injury imagery, visceral content) engages a separable processing channel. The cortical pain signature is readable by TRIBE v2; the subcortical component is not. The framework needs this dimension to distinguish pain-driven aversion from generally negative affect.
Thermal
The eliminating evidence is selective thermoreceptor loss - small-fiber neuropathy that eliminates temperature sensation while leaving touch and proprioception intact. The receptors for warmth (TRPV3/TRPV4 channels) and cold (TRPM8 channels) are molecularly separate from those for mechanical pressure (Piezo2 channels, as cataloged in Chapter 3 1.). The evidence is Moderate - the dissociation is well established but the experimental literature is smaller than for the more frequently studied modalities. Confidence tier: mixed - thermoreceptors at lower confidence, thermosensory cortex at higher confidence.
Khozai implication. Thermal engagement in video content is indirect (the predictive processing that produces a felt sense of cold from snowy imagery), but the dimension is included because the receptor system is real and the experiential aspect is structurally separable.
Proprioceptive
The eliminating evidence is patient IW (Cole, 1995) [8] - the case discussed in 2. under the Bodily dimension. IW lost large-fiber afferents from below the neck, eliminating proprioception (the felt sense of limb position) while leaving pain and temperature sensation intact. The dissociation is selective: the receptors for limb position (muscle spindles and Golgi tendon organs, Chapter 3 1.) are anatomically separate from those for pain, temperature, and crude touch. The evidence is Strong, resting on this single well-characterized case extended by subsequent similar cases. Confidence tier: mixed - spinal proprioceptive pathways at lower confidence, somatosensory cortex representation at higher confidence.
Khozai implication. Proprioceptive engagement in video content is indirect, mediated by the mirror system and predictive processing when watching others move. The dimension is named explicitly to prevent collapsing it with Tactile or Bodily-as-a-whole.
Vestibular
The eliminating evidence is bilateral vestibulotomy - surgical destruction of the vestibular organs in both inner ears, performed historically as a treatment for severe Meniere’s disease. Affected individuals lose the felt sense of head orientation and motion in space while retaining vision, hearing, and all body sensation outside the vestibular receptor system. The evidence is Strong. Confidence tier: lower (peripheral vestibular organ; cortical vestibular representation is distributed and less well characterized than other sensory areas).
Khozai implication. Vestibular engagement in video content is indirect except for content specifically designed to induce vection (the felt sense of self-motion produced by full-field visual motion, as in immersive content). Naming Vestibular as a separable dimension prevents reading vection responses as proprioceptive or generally arousing.
Olfactory
The eliminating evidence is anosmia - loss of smell from olfactory nerve damage, often through head trauma severing the olfactory nerve at the cribriform plate (the perforated bone separating the nasal cavity from the brain). Affected individuals lose smell while retaining all other sensory modalities. The evidence is Strong. Confidence tier: higher (olfactory cortex is cortical surface, though less studied by brain encoding models than visual or auditory cortex).
Gustatory
The eliminating evidence is ageusia - loss of taste from chorda tympani nerve damage or other peripheral lesions affecting taste receptors and their afferent pathways. The dissociation from olfaction is partial in everyday experience (much of “flavor” is olfactory) but well established at the receptor level: taste receptors and olfactory receptors are anatomically and molecularly distinct. The evidence is Strong. Confidence tier: higher (gustatory cortex in the insula is cortical surface).
Khozai implication. Both Olfactory and Gustatory engagement are essentially absent from screen-mediated video content. The dimensions are included because the framework’s claim to span Experience Space requires that it not arbitrarily exclude sensory channels just because the current measurement context does not engage them - the dimension set is defined by neurology, not by measurement context.
Interoceptive
The eliminating evidence comes from insular cortex damage - specifically, lesions to the anterior insular cortex that produce reduced awareness of internal body state, including reduced perception of heart rate, breathing, gut state, and other visceral signals. The seminal review is the neuroanatomist A.D. Craig [10] (Nature Reviews Neuroscience), which characterized the anterior insula as the cortical site for interoceptive awareness; subsequent fMRI and lesion work has supported the role. The evidence is Moderate - the dissociation is consistent across studies but the experimental literature is smaller and the interpretation more contested than for the primary sensory modalities. Confidence tier: higher (anterior insular cortex is cortical surface), but the visceral afferent pathways feeding it are subcortical (lower confidence).
A naming reconciliation applies here. The receptor system that supplies the body-state signal is visceral afferents - the sensory nerves carrying mechanoreceptive, chemoreceptive, and osmoreceptive information from internal organs (Chapter 2, Premise 2; Chapter 3 1.). The experiential dimension that those signals contribute to, when processed by anterior insula and other interoceptive cortical regions, is called Interoceptive here. Both names are correct; they refer to different things. This chapter uses Interoceptive consistently for the dimension from this point forward.
Khozai implication. Interoceptive engagement in video content is indirect but real. Content that triggers visceral responses (anxiety-provoking material, visceral disgust imagery, food content that produces hunger) engages the Interoceptive dimension through predictive processing rather than through direct visceral stimulation. Chapter 3 4. traced the body-state monitoring pathway and noted its confidence transition from lower (subcortical visceral afferents) to higher (insular cortex representation). TRIBE v2 can read the cortical endpoint but not the subcortical driver.
Eight Non-Sensory Dimensions at Resolution Level 2
Beyond the ten sensory modalities, eight further dimensions become separable at Resolution Level 2. They expand the Affective, Motivational, and Cognitive aspects from 2. by making explicit the components those broader dimensions contained.
| Dimension | Parent (RL1) | Eliminating evidence | Key study | Evidence rating | Confidence tier | Dissociation type (Tool 1) |
|---|---|---|---|---|---|---|
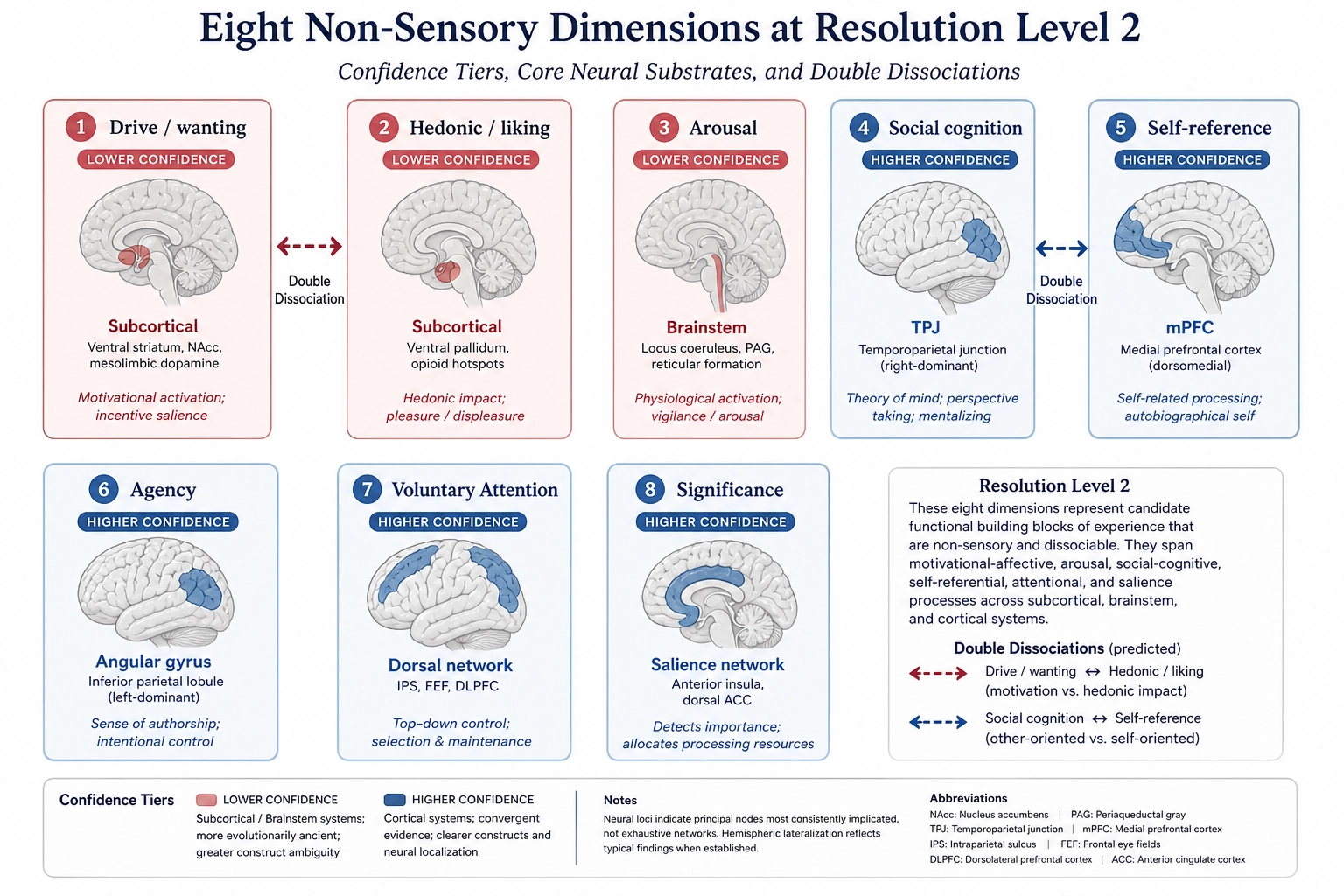
| Drive (wanting) | Motivational | Dopamine depletion in mesolimbic pathway | [3] | Strong | Lower (subcortical - VTA, ventral striatum) | Double - with Hedonic |
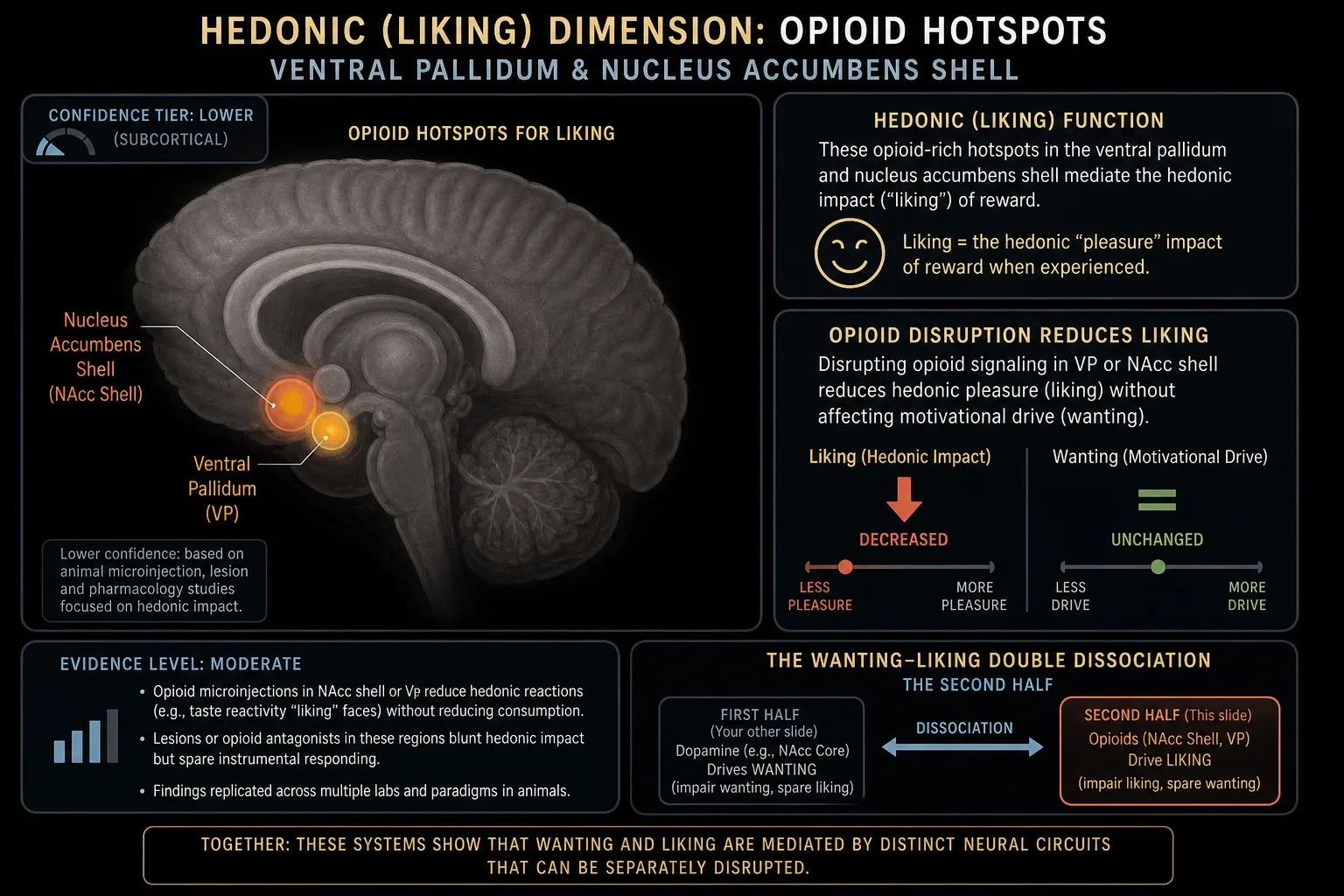
| Hedonic (liking) | Motivational | Opioid system disruption | [3] | Moderate | Lower (subcortical - opioid hotspots in ventral pallidum) | Double - with Drive |
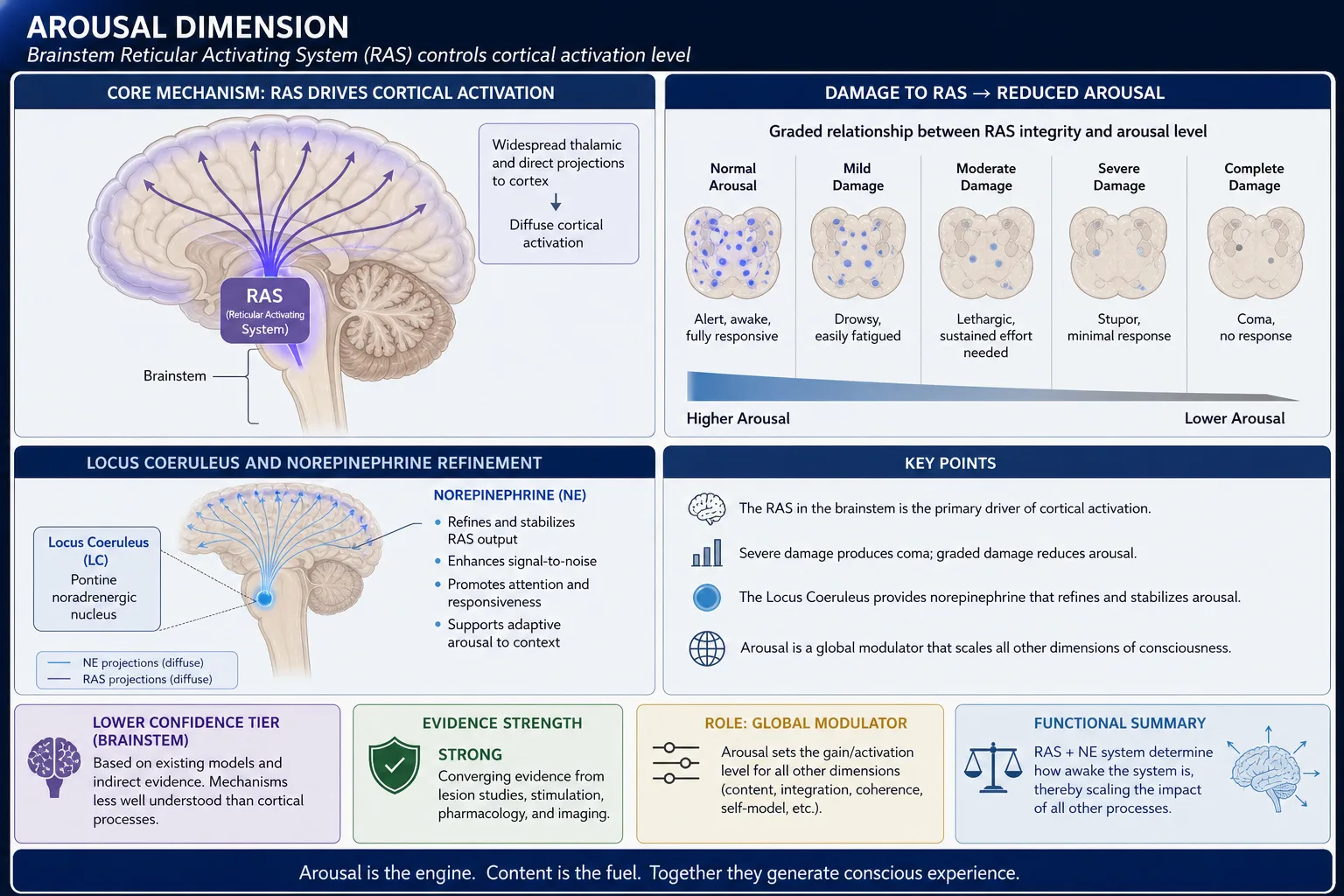
| Arousal | Affective/Global | Brainstem RAS damage | [21] | Strong | Lower (brainstem) | Single - arousal reduced, content preserved |
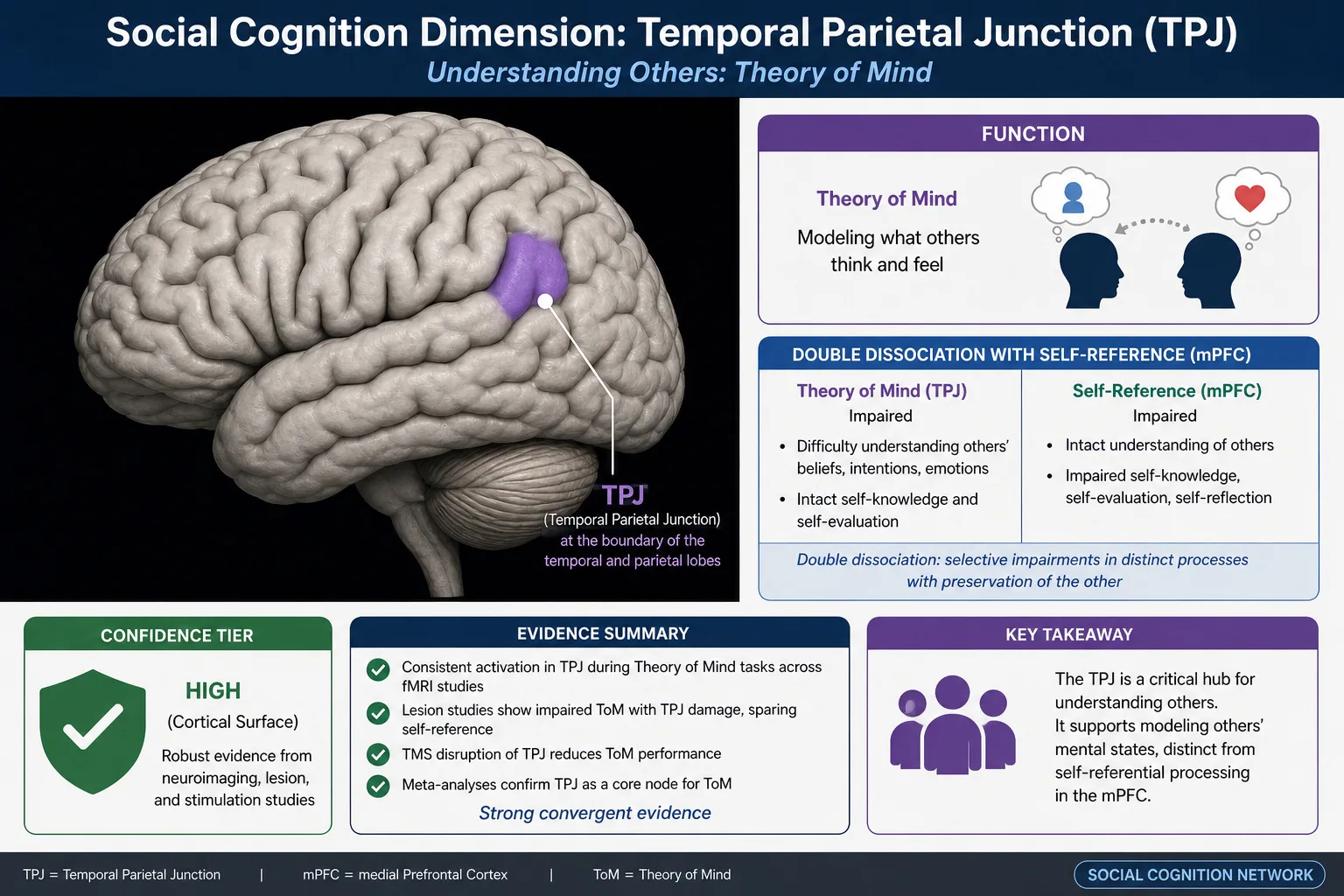
| Social cognition | Cognitive | TPJ damage | [25] | Strong | Higher (cortical - TPJ) | Double - with Self-reference |
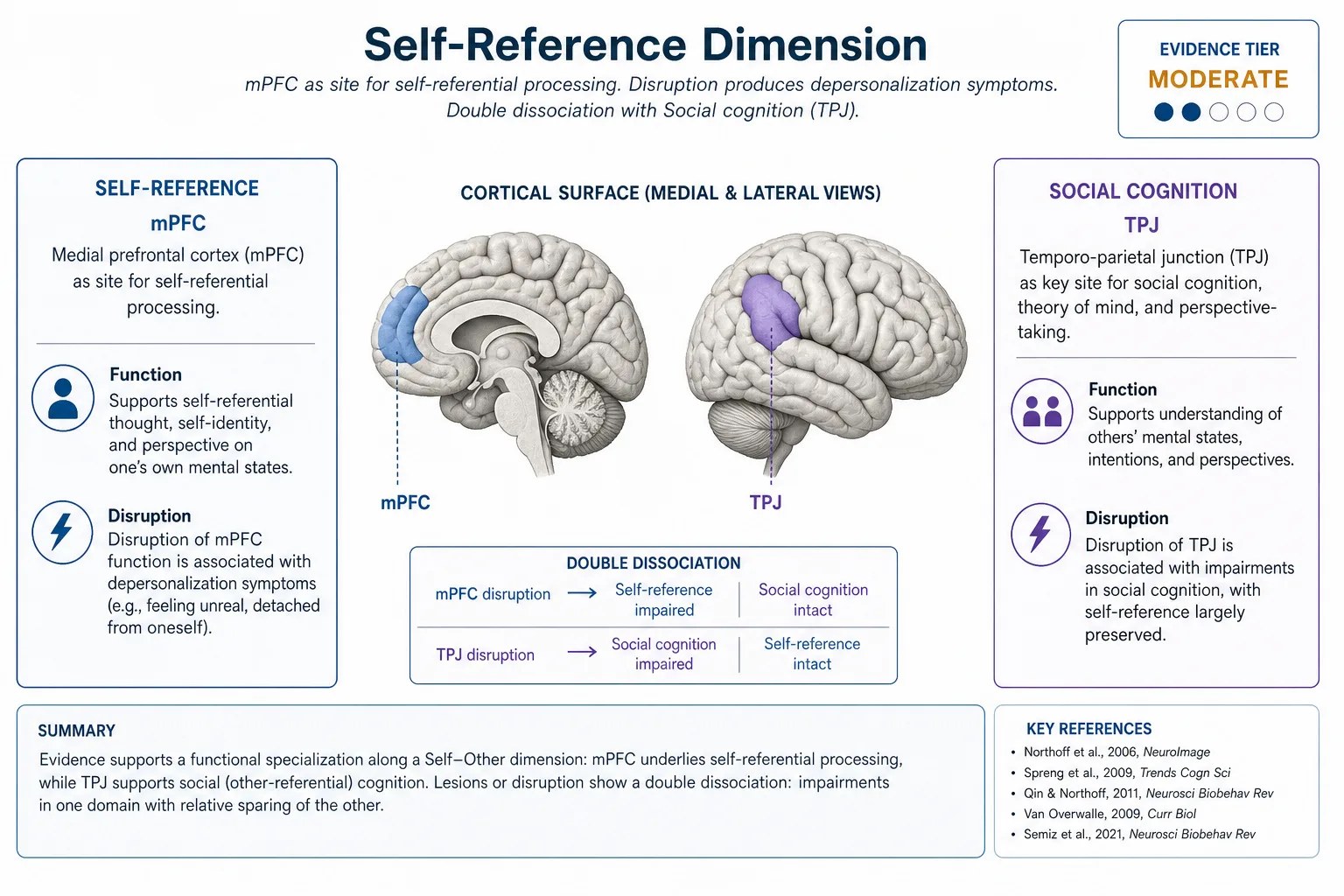
| Self-reference | Cognitive | mPFC disruption | [23] | Moderate | Higher (cortical - mPFC) | Double - with Social cognition |
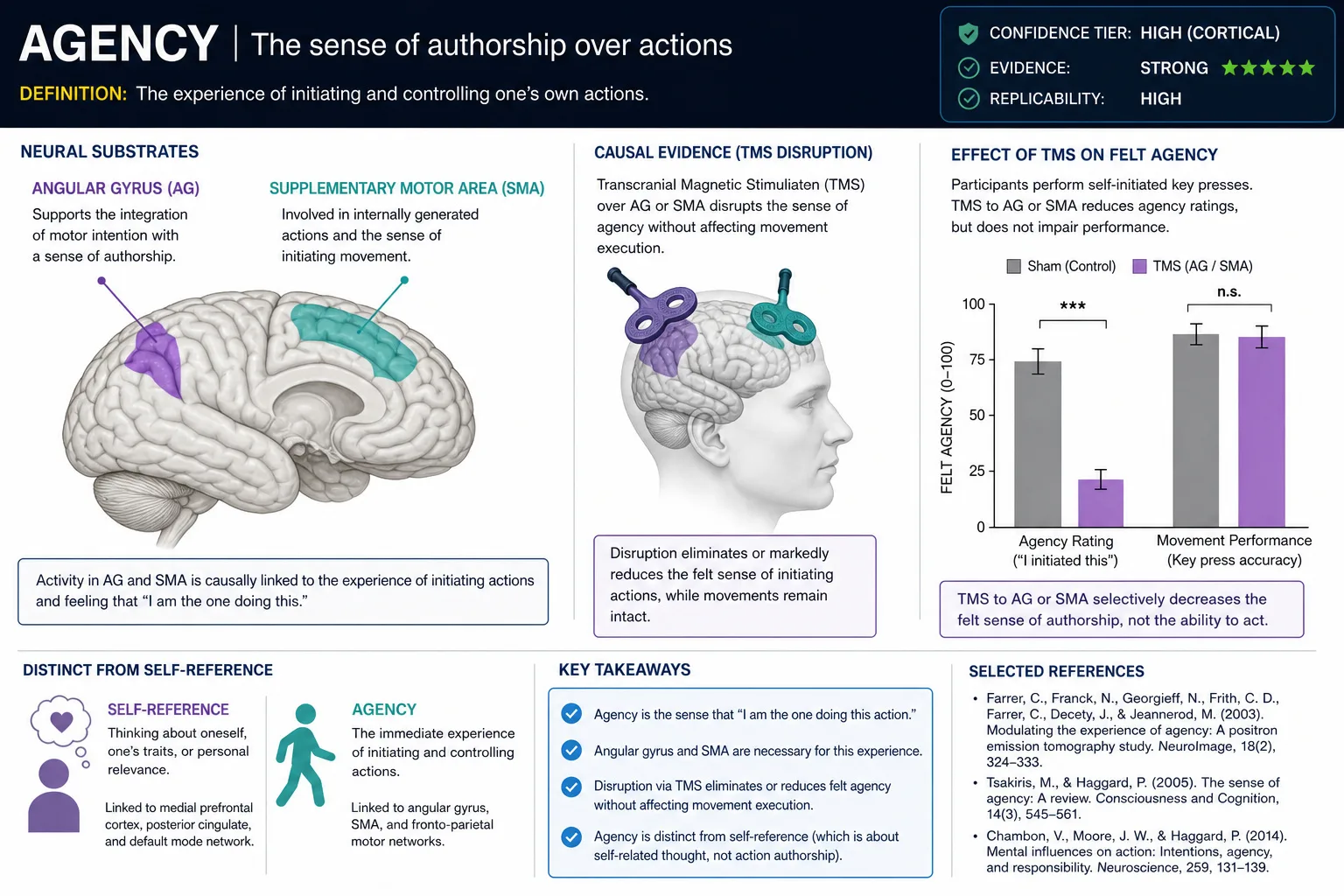
| Agency | Cognitive/Bodily | Angular gyrus + SMA disruption | [16] | Strong | Higher (cortical - angular gyrus, SMA) | Single - agency lost, action preserved |
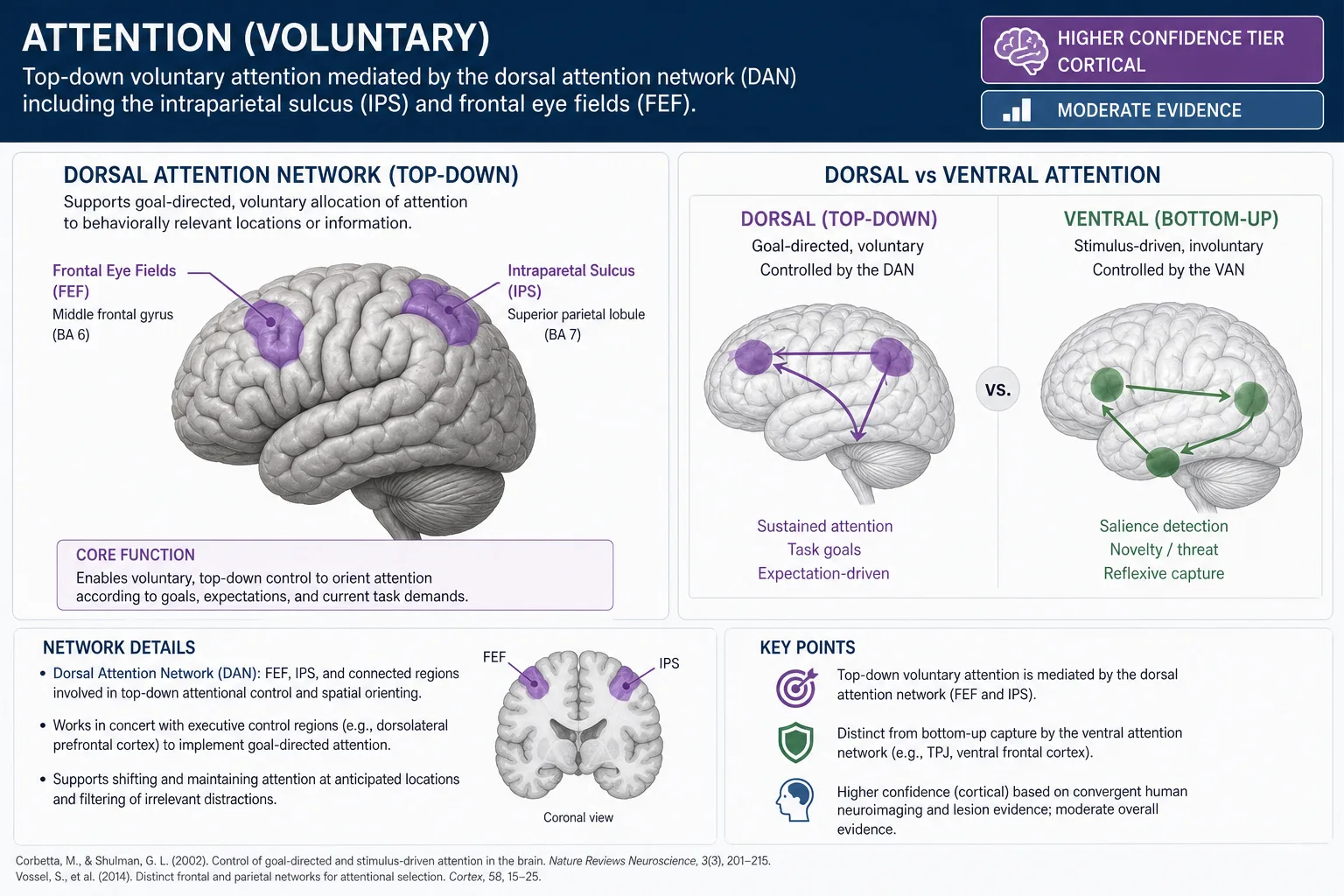
| Attention (voluntary) | Cognitive | Dorsal attention network damage | [9] | Moderate | Higher (cortical - IPS, FEF) | Single - voluntary control impaired, stimulus-driven intact |
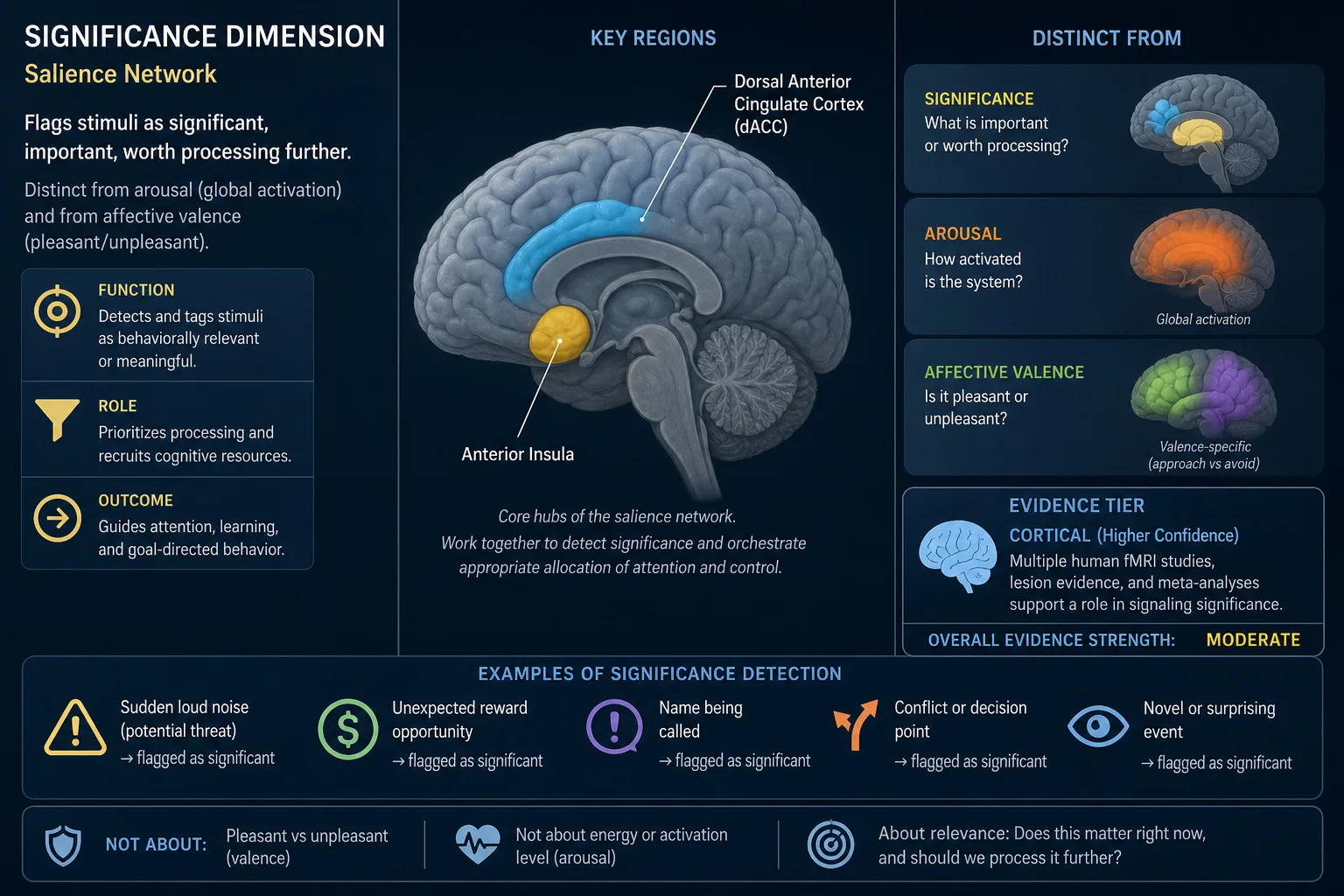
| Significance | Affective/Cognitive | Salience network disruption (AI + dACC) | [27] | Moderate | Higher (cortical - anterior insula, dACC) | Single - salience detection impaired |
Drive (wanting)
The eliminating evidence is the dopamine-depletion side of the wanting-liking double dissociation described in 2. Motivational above (Berridge & Robinson [3]). The evidence is Strong. Confidence tier: lower (subcortical - VTA and ventral striatum are not directly readable by cortical encoding models).
Khozai implication. Drive is what makes a viewer keep watching, click through, return for more. It is the dimension most directly tied to retention and follow-through behavior - and it sits in Khozai’s blind spot. TRIBE v2 cannot directly predict mesolimbic dopamine activity. The framework is designed to infer Drive from two sources: cortical correlates (prefrontal goal-representation activity, which is readable) and Vp (behavioral signals like watch-through rate and return visits, which are directly measured). When the framework reports “high retention,” the Drive dimension is the experiential axis most likely responsible, but the inference is indirect.
Hedonic (liking)
The eliminating evidence is the opioid-disruption side of the wanting-liking double dissociation described in 2. Motivational above (Berridge & Robinson [3]): opioid antagonists reduce hedonic response while leaving wanting intact. The evidence is Moderate - strong for the dissociation itself, slightly less established than the wanting side because the opioid manipulations are more pharmacologically complex. Confidence tier: lower (subcortical - opioid hotspots in the ventral pallidum and nucleus accumbens shell).
Khozai implication. Hedonic engagement is the felt pleasantness or unpleasantness of a content piece in the moment of consumption. A content piece can be strongly Drive-engaging (compulsive to keep watching) without being strongly Hedonic (pleasant); the reverse is also possible. Like Drive, Hedonic sits at lower confidence - the opioid hotspots are subcortical. The framework can infer hedonic response from cortical valence signatures (orbitofrontal cortex, readable by TRIBE v2) and from self-report in Vp, but the direct subcortical hedonic signal is not readable.
Arousal
The eliminating evidence is damage to the brainstem reticular activating system (RAS) - the brainstem network whose activity determines whether the cortex is online at all. Severe RAS damage produces coma; graded damage produces graded reduction in arousal. The seminal characterization is the neurophysiologists Giuseppe Moruzzi and Horace Magoun [21]. Subsequent work has refined the picture (Aston-Jones & Cohen [2], on the locus coeruleus and norepinephrine) but the basic dissociation has held: arousal can be reduced selectively, with content of experience preserved at lower vividness, until arousal goes low enough to extinguish consciousness entirely. The evidence is Strong. Confidence tier: lower (brainstem - not predictable from cortical-only encoding models).
Khozai implication. Arousal is a global modulator that scales every other dimension. Content properties (motion energy, audio amplitude, cut rate) drive arousal somewhat independently of which other dimensions they engage. Arousal regulation is a brainstem function, and brainstem activity is not predictable from cortical-only models like TRIBE v2. The framework can name Arousal as a dimension and reason about it through cortical correlates (cortical arousal signatures are partially readable) and behavioral signatures (pupil dilation, skin conductance in lab settings; engagement duration in platform settings), but cannot directly read brainstem arousal from a cortical activation prediction. Chapter 3 3. classified the RAS as infrastructure with lower confidence; that classification carries directly into this dimension. Chapter 11 will return to this under TRIBE v2’s blind spots.
Social cognition
The eliminating evidence is damage to the temporal parietal junction (TPJ) - the cortical region at the boundary of the temporal and parietal lobes that the social cognition literature has identified as central to theory of mind, the capacity to model what others are thinking and feeling. Patients with right TPJ damage show selective impairment of theory-of-mind tasks (false-belief reasoning, intention attribution) while retaining self-referential processing, perception, and other cognitive capacities. The dissociation from Self-reference is double: TPJ damage impairs social cognition but preserves self-reference; mPFC damage impairs self-reference but preserves social cognition (the cognitive neuroscientists Rebecca Saxe and Nancy Kanwisher [25], NeuroImage 19(4):1835-1842; the neuroscientist Georg Northoff and colleagues [23]). The evidence is Strong. Confidence tier: higher (cortical surface - TPJ is directly readable by TRIBE v2).
Khozai implication. Social cognition engagement is what is happening when a viewer interprets the intentions, beliefs, and feelings of people on screen. Content with characters whose mental states are being modeled - narrative content, interpersonal content, content with faces that read as having intent - engages this dimension. Because TPJ sits at higher confidence, TRIBE v2 can predict social-cognitive cortical activation from content features. This makes Social cognition one of the dimensions where the framework’s measurement is most direct. Vc (the content representation vector) is designed to detect social content; Vn to predict the cortical response; Ve to estimate the experiential result.
Self-reference
The eliminating evidence is disruption of the medial prefrontal cortex (mPFC) - the region most consistently identified with self-referential processing in meta-analyses (Northoff et al. [23], NeuroImage 31(1):440-457). Disruption produces depersonalization-like symptoms in which the patient retains social cognition (modeling others) but loses the felt sense that experience is happening to them, that memories belong to them, that thoughts are theirs. Stendardi and colleagues [37] (2021) demonstrated in Social Cognitive and Affective Neuroscience that vmPFC lesion patients showed an abolished self-reference effect in memory: they no longer encoded self-relevant information better than other-relevant information, while brain-damaged controls retained the effect. A clarification: basic self-awareness is preserved after vmPFC damage (as Philippi et al., 2012, showed), but the quality and encoding advantage of self-referential processing is impaired. The double dissociation with Social cognition (see above) is established: mPFC damage disrupts self-reference but not social cognition; TPJ damage disrupts social cognition but not self-reference. The evidence is Moderate - strong for the mPFC role, more contested for the precise boundaries of the dimension. Confidence tier: higher (cortical surface - mPFC is readable by TRIBE v2).
Khozai implication. Self-reference is what is happening when a viewer relates content to their own life, sees themselves in a story, or processes content as personally relevant. The dimension is critical for content that depends on relatability. Because mPFC sits at higher confidence, the framework is designed to estimate self-referential engagement from brain encoding predictions. The dissociation from Social cognition matters operationally: a content piece can engage one without the other, and the behavioral consequences differ (self-referential engagement predicts personal sharing; social-cognitive engagement predicts discussion about others).
Agency
The eliminating evidence is disruption of the angular gyrus and supplementary motor area (SMA) - cortical regions involved in the sense of authorship over actions - producing a loss of the sense of agency, the felt experience of one’s actions being one’s own. Affected individuals retain the ability to perform actions but lose the felt sense that they initiated them; the actions feel external, automatic, or as if controlled by another. The evidence comes from neurological case series and experimental disruption via transcranial magnetic stimulation (TMS), a non-invasive technique that uses magnetic pulses through the scalp to briefly perturb activity in a targeted cortical region (the neuroscientist Patrick Haggard [16], Nature Reviews Neuroscience 18:196-207, provides the comprehensive review). The evidence is Strong. Confidence tier: higher (cortical surface - angular gyrus and SMA are readable by TRIBE v2).
Khozai implication. Agency engagement is largely indirect in passive video viewing - viewers are not acting on the content. Agency becomes more relevant in interactive content (games, choose-your-own-adventure, second-screen interactions) and in content that simulates first-person agency through camera perspective and action. Naming Agency as a separable dimension prevents collapsing it with Self-reference, which it is distinct from despite frequent co-occurrence. Both sit at higher confidence, but they activate different cortical regions.
Attention (voluntary)
The eliminating evidence is disruption of the dorsal attention network - a cortical network including the intraparietal sulcus (IPS) and frontal eye fields (FEF) that the attention literature has identified as the substrate of top-down, voluntary attention (the neuroscientists Maurizio Corbetta and Gordon Shulman [9], Nature Reviews Neuroscience 3:201-215). This is the kind of attention a person directs intentionally, distinct from bottom-up, stimulus-driven capture (which is mediated by the ventral attention network). Damage to the dorsal network produces deficits in voluntary attentional control while leaving stimulus-driven attention relatively intact. Fernandez and colleagues [35] (PNAS, 2023) provided a clean experimental demonstration: transcranial magnetic stimulation to the right frontal eye field selectively disrupted endogenous (voluntary) attention while preserving stimulus-driven attention, a double dissociation between the two attentional systems produced by targeted cortical perturbation. The evidence is Moderate. Confidence tier: higher (cortical surface - IPS and FEF are readable by TRIBE v2).
Khozai implication. Voluntary Attention is what a viewer brings to content when they choose to watch carefully versus letting it play in the background. The framework distinguishes this from stimulus-driven attentional capture, which is an automatic response to physical properties (motion, contrast, sudden onset) and is driven by V0 properties rather than by the viewer’s intent. The Attention dimension, uniquely, is partly under viewer control rather than fully content-driven - two viewers watching identical content can differ on this axis. TRIBE v2 predicts average attentional response, not individual variation.
Significance
The eliminating evidence is disruption of the anterior insula and dorsal anterior cingulate cortex (dACC) - the salience network (the neurologist William Seeley and colleagues [27], Journal of Neuroscience 27(9):2349-2356), the cortical regions that flag a stimulus as significant, important, worth processing further. Disruption produces impaired salience detection: difficulty with the felt sense that something matters. The clinical pattern is visible in behavioral variant frontotemporal dementia (bvFTD): Seeley [36] (2010) showed in Brain Structure and Function that patients with frontoinsular degeneration lose the felt sense that things matter while retaining language and visuospatial function, a selective erosion of significance processing. The evidence is Moderate. Confidence tier: higher (cortical surface - anterior insula and dACC are readable by TRIBE v2).
Khozai implication. Significance is the felt importance of a content piece - distinct from Arousal (which is global activation) and distinct from Affective valence (which is pleasant/unpleasant). A content piece can be high in arousal, low in valence, and still feel insignificant; or low in arousal and high in significance. The salience network sits at higher confidence, making this dimension readable by TRIBE v2. This is operationally important: significance predicts whether content gets remembered and shared, which are key Vp outcomes. The dimension’s cortical readability means the framework is designed to predict significance-driven behavioral outcomes more directly than it can predict arousal-driven or drive-driven outcomes.
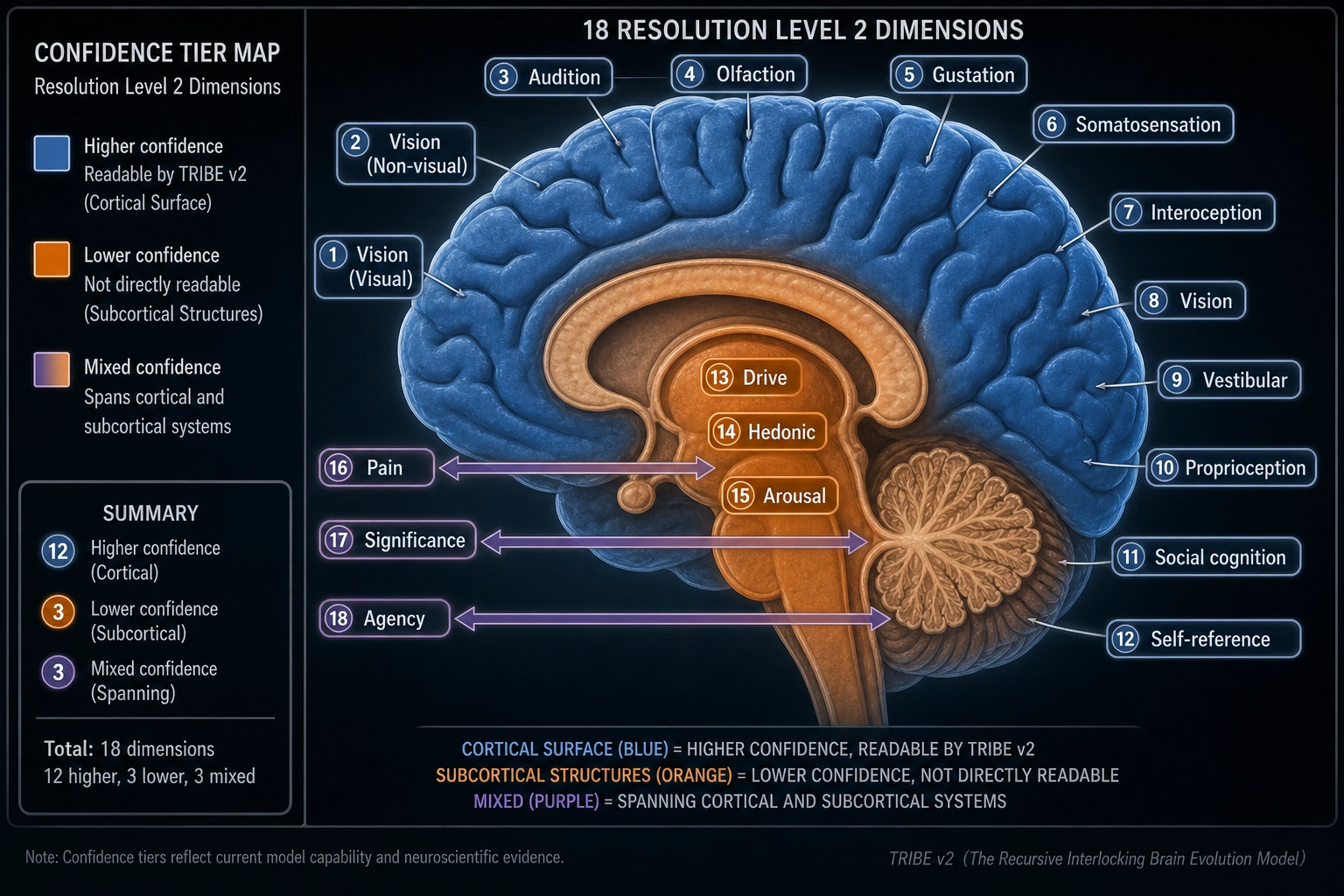
That completes the eighteen dimensions of Resolution Level 2: ten sensory modalities and eight non-sensory dimensions. Each is supported by selective elimination evidence; each is structurally separable from the others; each has its own evidence-quality rating, confidence tier, and specific implication for what Khozai can and cannot read from a viewer’s response. Of the eighteen, eleven sit at higher confidence (cortical surface, readable by TRIBE v2): six sensory modalities (Visual, Auditory, Tactile, Olfactory, Gustatory, Interoceptive) plus five non-sensory dimensions (Social cognition, Self-reference, Agency, Attention, Significance). Four sit at lower confidence (subcortical drivers): Vestibular, Drive, Hedonic, and Arousal. Three have mixed profiles where the cortical endpoint is readable but the subcortical driver is not: Pain, Thermal, and Proprioceptive. The framework is not uniformly confident across all dimensions, and it names the asymmetry.
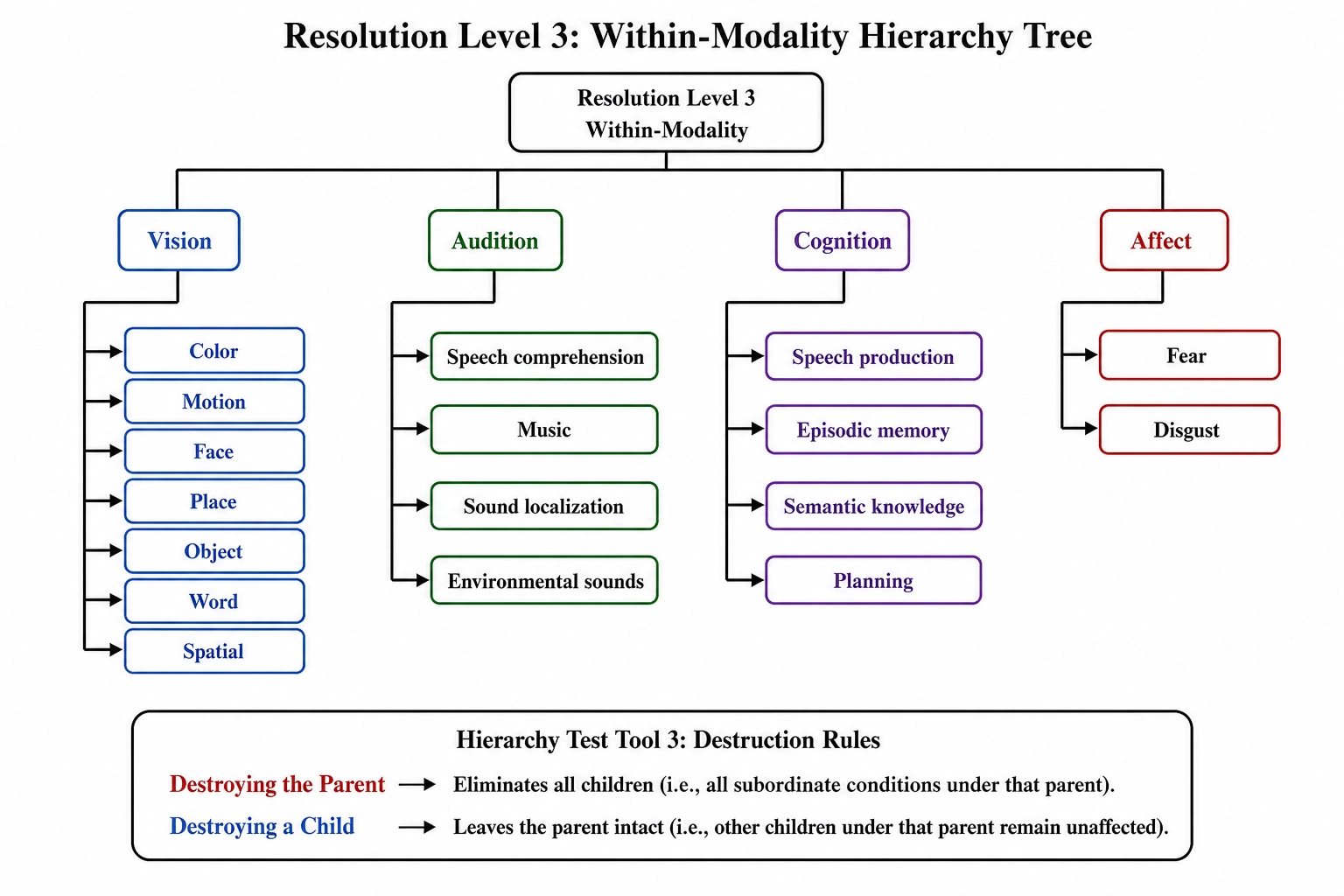
4. Resolution Level 3: Within-Modality Separations
At still finer resolution, several dimensions split further. The within-modality separations enumerated in Chapter 2 2..3 are reproduced here with their elimination evidence and their implication for Khozai. Seventeen sub-dimensions are enumerated in v1 (seven within Vision, four within Audition, four within Cognition, two within Affect). Combined with the fourteen RL2 dimensions that do not split further at this resolution, the enumerated total is thirty-one. The count is open at the bottom: additional dissociations can be discovered, and the dimension set grows with evidence. The Hierarchy Test (Tool 3) governs every split: the child dimension is eliminated when the parent’s substrate is destroyed, but the parent survives when only the child’s substrate is destroyed.
| Parent | Child dimension | Lesion site | Condition name | Key study | Evidence | Confidence |
|---|---|---|---|---|---|---|
| Visual | Color | V4 | Achromatopsia | [31] | Strong | Higher |
| Visual | Motion | MT/V5 | Akinetopsia | [33] | Strong | Higher |
| Visual | Face recognition | FFA (fusiform) | Prosopagnosia | [18] | Strong | Higher |
| Visual | Place/scene | PPA (parahippocampal) | Topographagnosia | [13] | Strong | Higher |
| Visual | Object recognition | Inferotemporal cortex | Visual agnosia | [14] | Strong | Higher |
| Visual | Word recognition | VWFA (left fusiform) | Pure alexia | [12] | Strong | Higher |
| Visual | Spatial awareness | Right parietal cortex | Hemispatial neglect | [20] | Strong | Higher |
| Auditory | Speech comprehension | Posterior temporal (Wernicke’s area) | Wernicke’s aphasia | [32] | Strong | Higher |
| Auditory | Music perception | Superior temporal gyrus | Amusia | [24] | Strong | Higher |
| Auditory | Sound localization | Planum temporale | Auditory spatial deficit | [30] | Strong | Higher |
| Auditory | Environmental sounds | Bilateral temporal cortex | Auditory agnosia | [7] | Moderate | Higher |
| Cognitive | Speech production | Inferior frontal (Broca’s area) | Broca’s aphasia | [4] | Strong | Higher |
| Cognitive | Episodic memory | Hippocampus | Amnesia | [26] | Strong | Mixed (hippocampus) |
| Cognitive | Semantic knowledge | Anterior temporal lobe | Semantic dementia | [17] | Strong | Higher |
| Cognitive | Planning/sequencing | Dorsolateral PFC | Dysexecutive syndrome | [28] | Strong | Higher |
| Affective | Fear | Amygdala (bilateral) | Selective fear loss | [1] | Strong | Lower (subcortical) |
| Affective | Disgust | Insular cortex | Selective disgust loss | [6] | Moderate | Higher |
Within Vision
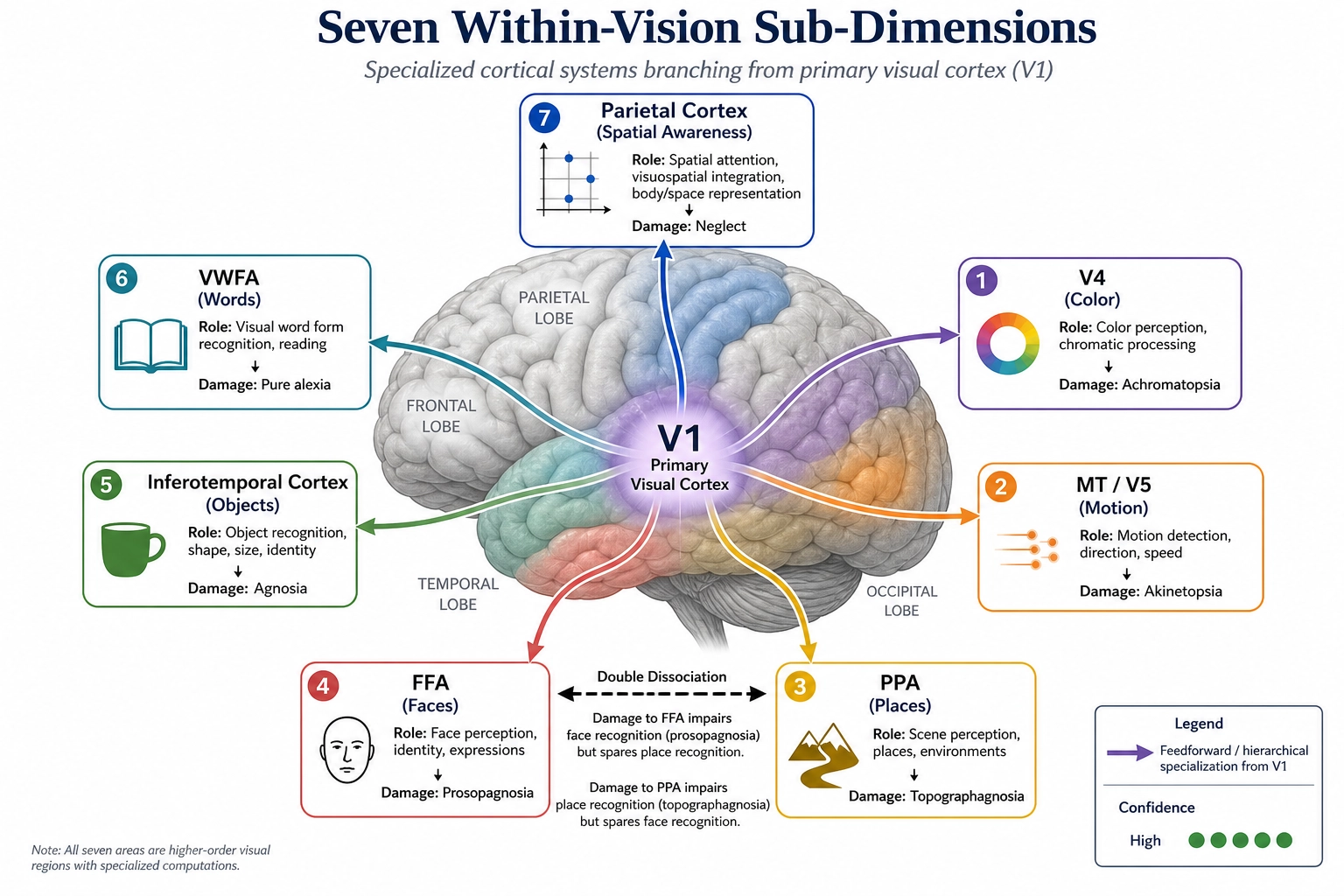
Color. Eliminated selectively by lesions to area V4 - a cortical area dedicated to color processing - producing achromatopsia, a loss of color vision while form, motion, and other visual processing remain intact (the neuroscientist Semir Zeki [31]). Patients see the world in shades of grey but retain spatial layout, motion perception, and object recognition. Hierarchy Test (Tool 3): destroying V1 (the parent) eliminates color along with all other vision; destroying V4 (the child) eliminates only color. The evidence is Strong. Confidence tier: higher (V4 is cortical surface, readable by TRIBE v2). The specificity of V4 for color perception is debated; V4 also responds to shape and texture (Roe et al., 2012), though selective achromatopsia cases confirm that color processing depends critically on this region. For Khozai, color is structurally separable from the rest of vision: a content piece’s color properties (spectral power distribution, hue, saturation) drive a specific cortical channel whose activation can be predicted independently of other visual channels.
Motion. Eliminated selectively by lesions to area MT/V5 - a cortical area dedicated to motion processing - producing akinetopsia, the loss of motion perception while form and color remain intact. The classic case (the neuropsychologist Josef Zihl and colleagues [33], Brain 106(2):313-340) describes a patient who saw the world in still frames: she could not pour tea because the liquid appeared to be frozen at one level then suddenly at another. Hierarchy Test (Tool 3): V1 destruction eliminates motion along with everything else visual; MT/V5 destruction eliminates only motion. The evidence is Strong. Confidence tier: higher (MT/V5 is cortical surface). MT/V5 responds to flicker and texture boundaries as well as motion (Albright, 1984), though akinetopsia cases confirm its necessity for motion perception specifically. For Khozai, motion is a separable channel: content properties tied to motion (optical flow, cut rate, temporal change) drive a specific cortical area whose engagement can be predicted separately from color and form.
Face recognition. Eliminated selectively by lesions to the fusiform face area (FFA) - a cortical region in the fusiform gyrus dedicated to face processing - producing prosopagnosia, the inability to recognize faces while object recognition, scene recognition, and other visual abilities remain intact (the cognitive neuroscientist Nancy Kanwisher and colleagues [18]). The evidence is Strong. Confidence tier: higher (FFA is cortical surface). The expertise hypothesis (Gauthier et al., 1999) challenges face-specificity, arguing FFA responds to any category of visual expertise; however, the congenital prosopagnosia evidence favors a face-selective account. For Khozai, face engagement is a separable channel: face area, face position, and face properties drive a specific cortical structure whose activation can be predicted by TRIBE v2 independently of other visual properties.
Place and scene recognition. Eliminated selectively by lesions to the parahippocampal place area (PPA) - a cortical region dedicated to scene and place processing - producing topographagnosia, the loss of the ability to recognize specific places and scenes while face and object recognition remain intact (the neuroscientist Russell Epstein and Kanwisher [13]). The evidence is Strong. Confidence tier: higher (PPA is cortical surface). For Khozai, scene recognition is a separable channel: content properties tied to environmental layout and place identity drive a specific cortical area independent of face processing.
Object recognition. Eliminated selectively by inferotemporal cortical lesions producing visual agnosia - the inability to recognize objects from their visual form while basic visual processing (color, motion, contour) remains intact (the cognitive neuroscientist Martha Farah [14]). The evidence is Strong. Confidence tier: higher (inferotemporal cortex is cortical surface). For Khozai, object recognition is a separable channel.
Word recognition. Eliminated selectively by lesions to the visual word form area (VWFA) - a region in left fusiform cortex specialized for orthographic processing - producing pure alexia, the inability to read while general visual processing and language comprehension remain intact (the neuroscientists Stanislas Dehaene and Laurent Cohen [12]). The evidence is Strong. Confidence tier: higher (VWFA is cortical surface). For Khozai, on-screen text engagement is a separable channel within vision; content with text drives a different cortical area than content without it.
Spatial awareness. Eliminated selectively by parietal lesions producing hemispatial neglect - the loss of awareness of one half of space while perceptual capacity in the affected hemifield is technically intact. Right parietal lesions classically produce left-side neglect (the neurologist M.-Marsel Mesulam [20]). The evidence is Strong. Confidence tier: higher (parietal cortex is cortical surface). For Khozai, the spatial framing of content (where elements sit in the frame) engages spatial processing channels separable from object identification.
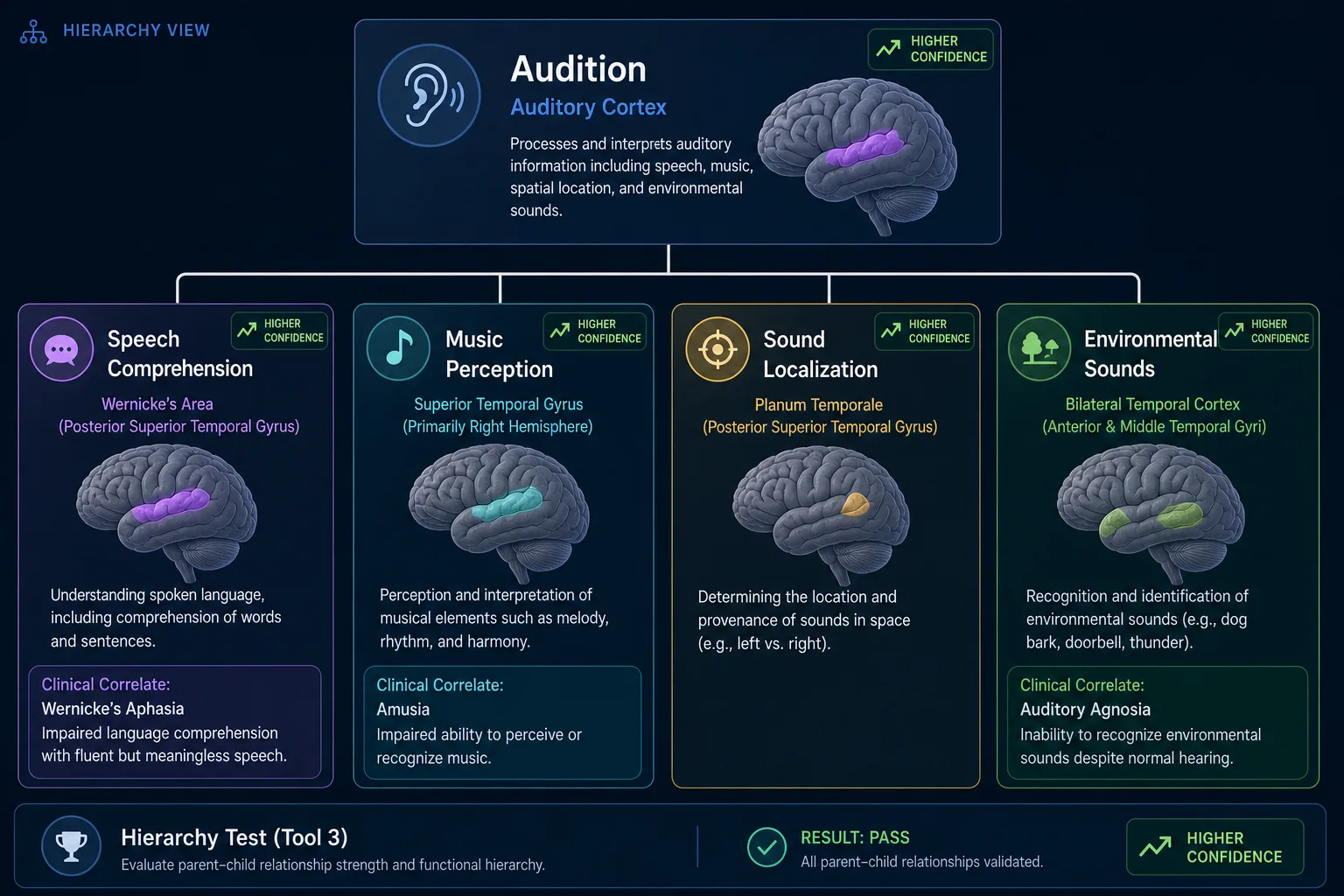
Within Audition
Speech comprehension. Eliminated selectively by posterior temporal lesions producing Wernicke’s aphasia - the loss of language comprehension while basic auditory processing remains intact. The dissociation from speech production (Broca’s aphasia) is the classical double dissociation in language neurology (Tool 1): Wernicke’s area damage removes comprehension but not production; Broca’s area damage removes production but not comprehension. The evidence is Strong. Confidence tier: higher (Wernicke’s area is cortical surface). For Khozai, speech engagement is a separable channel within audition; content with speech drives different cortical structures than content without it.
Music perception. Eliminated selectively by specific temporal lesions producing amusia - the loss of music perception while speech comprehension and other auditory abilities remain intact (the neuroscientist Isabelle Peretz and colleagues [24]). The evidence is Strong. Confidence tier: higher (superior temporal gyrus is cortical surface). Whether musical pitch processing is truly domain-specific or shares resources with speech prosody processing remains debated (Peretz and Coltheart, 2003), though double dissociations between amusia and aphasia support separability. For Khozai, music engagement is a separable channel.
Sound localization. Eliminated selectively by planum temporale lesions producing auditory spatial deficits - the loss of the ability to localize sounds in space while sound identification remains intact (the neuroscientists Robert Zatorre and Virginia Penhune [30]). The evidence is Strong. Confidence tier: higher (planum temporale is cortical surface). For Khozai, the spatial properties of audio (panning, depth cues) drive a separable channel within audition.
Environmental sound recognition. Eliminated selectively by bilateral temporal lesions producing auditory agnosia - the loss of the ability to recognize environmental sounds while music and speech may remain partially intact (Clarke and colleagues [7]). The evidence is Moderate. Confidence tier: higher (temporal cortex is cortical surface).
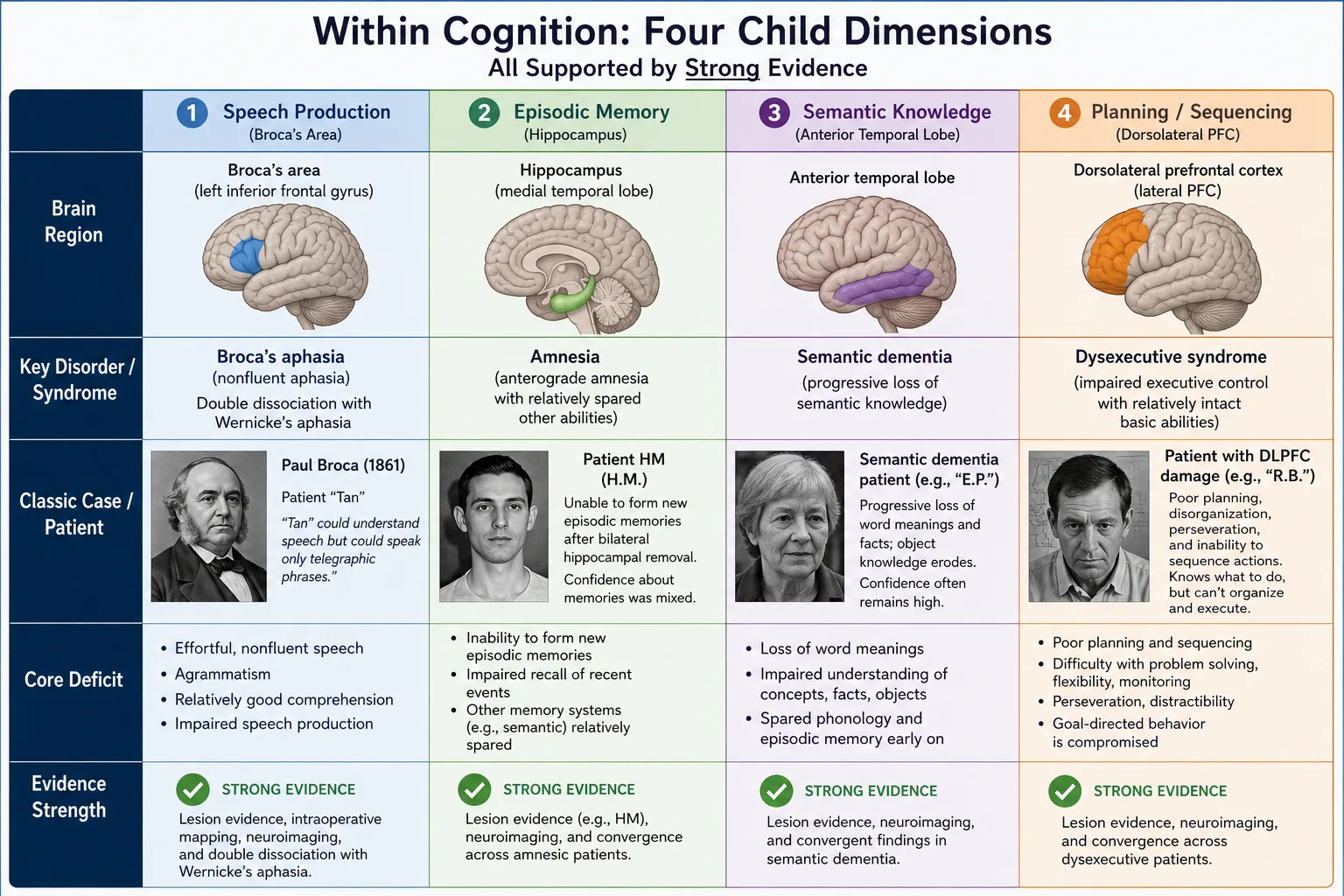
Within Cognition
Speech production. Eliminated selectively by inferior frontal lesions producing Broca’s aphasia - the loss of speech production while comprehension remains relatively intact. Double dissociation with Wernicke’s aphasia (Tool 1): Broca’s area damage removes production, Wernicke’s area damage removes comprehension. The evidence is Strong. Confidence tier: higher (Broca’s area is cortical surface).
Episodic memory. Eliminated selectively by hippocampal lesions producing amnesia. The classical case is patient HM (Henry Molaison), studied by Brenda Milner and colleagues for more than half a century after his bilateral medial temporal lobectomy in 1953 (Scoville & Milner [26] is the seminal report, as first introduced in Chapter 2). HM lost the ability to form new long-term episodic memories while retaining language, intelligence, perception, motor skills, short-term memory, and the ability to learn certain new motor procedures. What this chapter adds to Chapter 2’s account: the dissociation is extraordinary in its specificity because it demonstrates that a single structural lesion can produce a single experiential loss - the strongest possible evidence for the decomposition claim. The evidence is Strong. Confidence tier: mixed (the hippocampus is deep medial temporal, not cortical surface - TRIBE v2’s ability to predict hippocampal activity from cortical patterns is indirect and lower-confidence).
Semantic knowledge. Eliminated selectively by anterior temporal degeneration producing semantic dementia - the progressive loss of word meanings and conceptual knowledge while episodic memory, language fluency, and perception remain relatively preserved early in the disease (the neurologist John Hodges and colleagues [17]). Double dissociation with episodic memory (Tool 1): hippocampal damage removes episodic memory but spares semantic knowledge; anterior temporal degeneration removes semantic knowledge but spares episodic memory (early in the disease course). The evidence is Strong. Confidence tier: higher (anterior temporal cortex is cortical surface).
Planning and sequencing. Eliminated selectively by dorsolateral prefrontal lesions producing dysexecutive syndrome - the loss of complex planning and goal-directed sequencing while other cognitive functions remain intact (Shallice (1982) [28]). The evidence is Strong. Confidence tier: higher (dorsolateral PFC is cortical surface).
Within Affect
Fear specifically. Eliminated selectively in patient SM - the bilateral amygdala patient discussed in 2. (as established in Chapter 2 2..4 [1]) - fear is gone while other emotions remain intact and reportable. The case has been extended to a broader patient series and supplemented by fMRI work on amygdala function. The evidence is Strong. Confidence tier: lower (amygdala is subcortical - TRIBE v2 cannot directly predict amygdala activation from content features). For Khozai, fear is a separable channel within affect; content that engages fear (threat imagery, suspense) drives a specific subcortical structure whose engagement sits in the framework’s blind spot. Fear can be inferred from cortical correlates (prefrontal threat-processing signatures, which are readable) and from behavioral and self-report signatures in Vp, but the direct amygdala signal is not readable.
Disgust specifically. Eliminated selectively by insular lesions producing impaired disgust recognition and response while other emotional processing remains intact (the psychologist Andrew Calder and colleagues [6]). The evidence is Moderate. Confidence tier: higher (insular cortex is cortical surface, readable by TRIBE v2).
This is the level at which the dimension count reaches thirty-one (eighteen RL2 dimensions minus four that split, plus seventeen RL3 sub-dimensions). Resolution Level 3 is open at the bottom: future selective eliminations may discover additional separations within currently-named dimensions, and the framework treats this as a feature rather than a defect. The dimension set grows with evidence.
A practical implication. The thirty-one dimensions of Resolution Level 3 are too fine for many operational purposes. Resolution Level 2’s eighteen dimensions are the level at which the framework typically reasons about content - granular enough to capture meaningful structure, coarse enough to avoid drowning in dimensions that rarely vary independently in screen-mediated content. The framework leaves all three resolutions available simultaneously; coarser resolutions are projections of finer ones. All RL3 within-modality splits sit at higher confidence (cortical surface, readable by TRIBE v2) except two: Fear (amygdala, lower confidence) and Episodic memory (hippocampus, mixed confidence). This is consistent with the general pattern: the deeper the hardware sits beneath the cortical surface, the less directly the framework can predict its activation.
5. Psychological Constructs as Patterns
Psychology has been naming states for over a century. Anxiety, flow, nostalgia, awe, joy, grief, boredom, curiosity, contempt, affection. These names are useful - they pick out clusters that recur, that we recognize in ourselves and others, that organize how we talk about experience. But they are not dimensions in this framework. They are regions in dimension space - specific configurations of values across the dimensions already named. The Pattern Verification Test (Tool 4) makes the relationship explicit.
The procedure has four steps. Map the construct to specific values across existing dimensions. Test whether altering one component dimension shifts the experience out of the construct (if so, the construct is not atomic - it is a pattern). Test whether all components are necessary (if removing one transforms the experience away from the construct, it is a conjunction, not a sum). Test for residual - after accounting for all components, is anything left? If no residual, the construct is confirmed as a pattern.
| Construct | Arousal | Affective valence | Significance | Drive | Hedonic | Attention | Self-reference | Interoceptive | Episodic memory | Cognitive focus | Residual |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Anxiety | High | Negative | High | - | - | - | - | High | - | Threat-anticipatory | None |
| Flow | Moderate | - | Low (outside task) | High | Moderate-high | High (voluntary) | Low | Low | - | Task-focused | None |
| Nostalgia | Moderate | Mixed (bittersweet) | High (directed at recalled period) | - | - | - | High | - | High | Past-oriented | None |
| Awe | Elevated | Positive (can include fear) | High (vastness) | - | - | - | Low (“small self”) | - | - | Vastness-oriented | None |
Four constructs follow. Each is reconstructed as a configuration across dimensions, and the Pattern Verification Test (Tool 4) is shown for each.
Anxiety
Anxiety as a pattern decomposes approximately as: high Arousal, negative Affective valence (unpleasant), high Significance (something matters), Cognitive engagement focused on threat-related content (often anticipatory), and elevated Interoceptive activation (felt body signals - racing heart, tight chest, gut tension). The dimensions are not equally engaged in every instance, but the pattern recurs.
The test (Tool 4): pharmacologically reducing arousal alone with a beta-blocker reduces the felt arousal and visceral component, and the experience shifts out of the named state - it stops being recognizable as anxiety and becomes something more like worried thought without bodily activation, or vigilance without panic. The component dimensions are not identical to anxiety; their conjunction at specific values is. Removing any single one (for instance, eliminating the negative valence while keeping the rest produces something more like alertness or excitement; eliminating the cognitive threat-content while keeping the rest produces something more like physiological arousal without anxiety) shifts the experience out of the construct. There is no residual that requires positing an “anxiety dimension” beyond the configuration.
Khozai implication. Anxiety-engaging content can be characterized by the pattern of dimensional engagement it produces - and content properties can be designed or analyzed in terms of which components of the anxiety pattern they touch. Suspense scenes, for instance, drive Arousal and Significance heavily while keeping affective valence ambiguous; horror content drives the same plus negative Affective valence and elevated Interoceptive activation. The pattern view lets the framework reason about why two content pieces that both feel “anxious” might produce different behavioral outcomes if they engage different components of the underlying pattern. Measurement note: the Arousal and Interoceptive components sit at lower confidence (subcortical drivers); the Significance and Cognitive components sit at higher confidence (cortical). The framework is designed to read the cortical components directly and infer the subcortical ones.
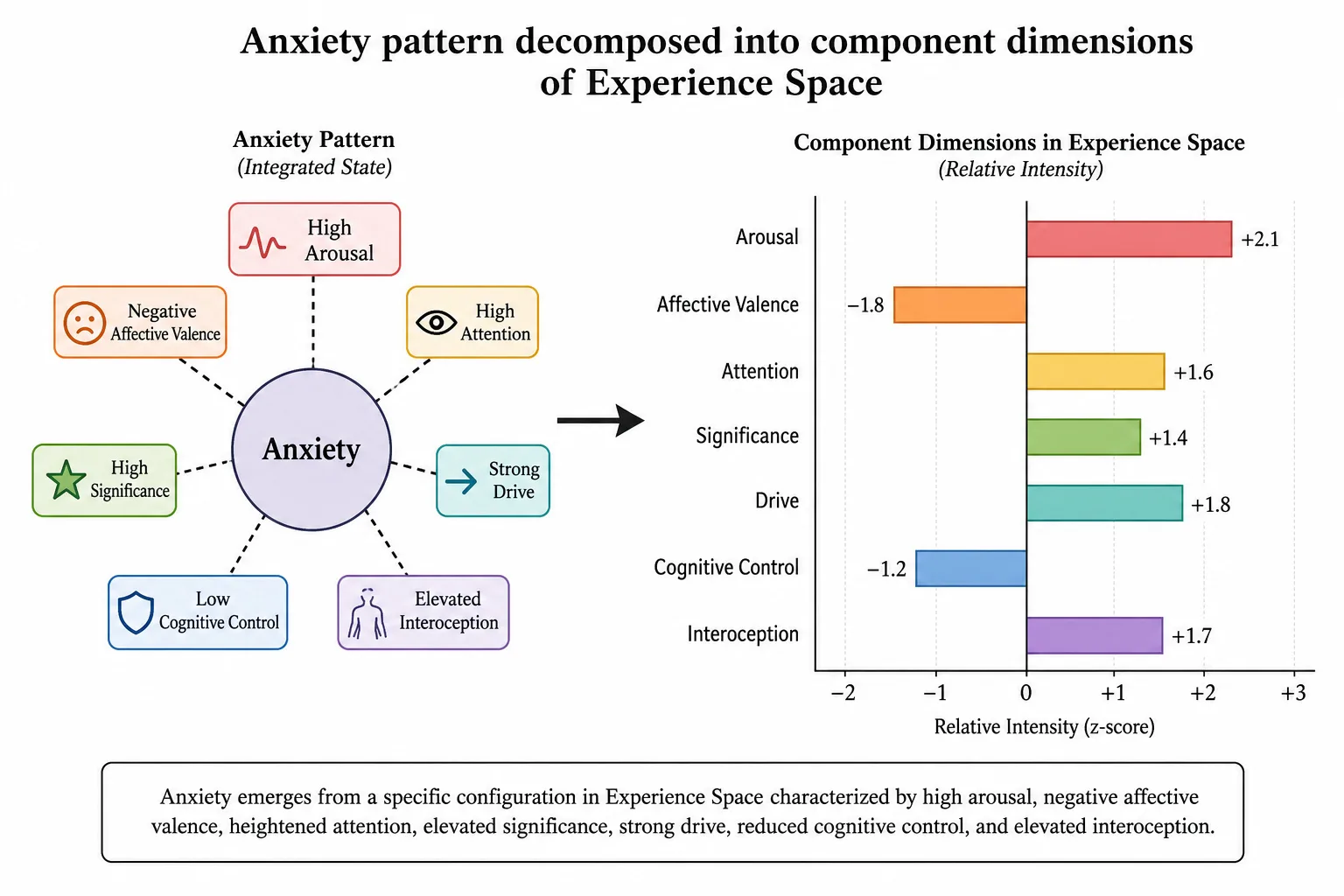
Flow
Flow as a pattern decomposes approximately as: high voluntary Attention focused on a single task or stimulus stream, high Drive (the activity is pulling), moderate to high Hedonic engagement (the activity is felt as good), low Self-reference (attenuated awareness of self as separate from activity), and a specific pattern of reduced Significance for everything outside the focal task. Awareness of time and bodily state typically attenuates as well.
The test (Tool 4): experimentally disrupting voluntary attention (by introducing distraction) shifts the experience out of flow even if every other component remains. The psychologists C. Marr and Jan Theeuwes [38] (2018) showed in Cognitive, Affective, & Behavioral Neuroscience that flow depends on complete mobilization of attentional resources, and Harris, Vine, and Wilson [39] (2017) reviewed in Progress in Brain Research how flow states require sustained frontoparietal network engagement: disrupting that engagement breaks the state. Similarly, increasing self-reference (by making the participant self-conscious about the task) collapses flow into something more like effortful performance. The construct decomposes into components that can be selectively perturbed; no residual remains.
Khozai implication. Content that engages flow tends to be content with high enough cognitive demand to require sustained voluntary attention but not so high that it produces frustration - the sweet spot the flow literature has long described (the psychologist Mihaly Csikszentmihalyi [11], Flow: The Psychology of Optimal Experience, Harper & Row; Nakamura & Csikszentmihalyi [22]). The framework is designed to read flow in terms of which dimensions are engaged at what magnitudes, which decouples the construct from any one content category and lets the analysis transfer across formats. Measurement note: the Attention and Self-reference components sit at higher confidence (cortical); the Drive component sits at lower confidence (subcortical). Flow’s behavioral signature in Vp - long, uninterrupted watch sessions without seeking behavior - provides a complementary signal.
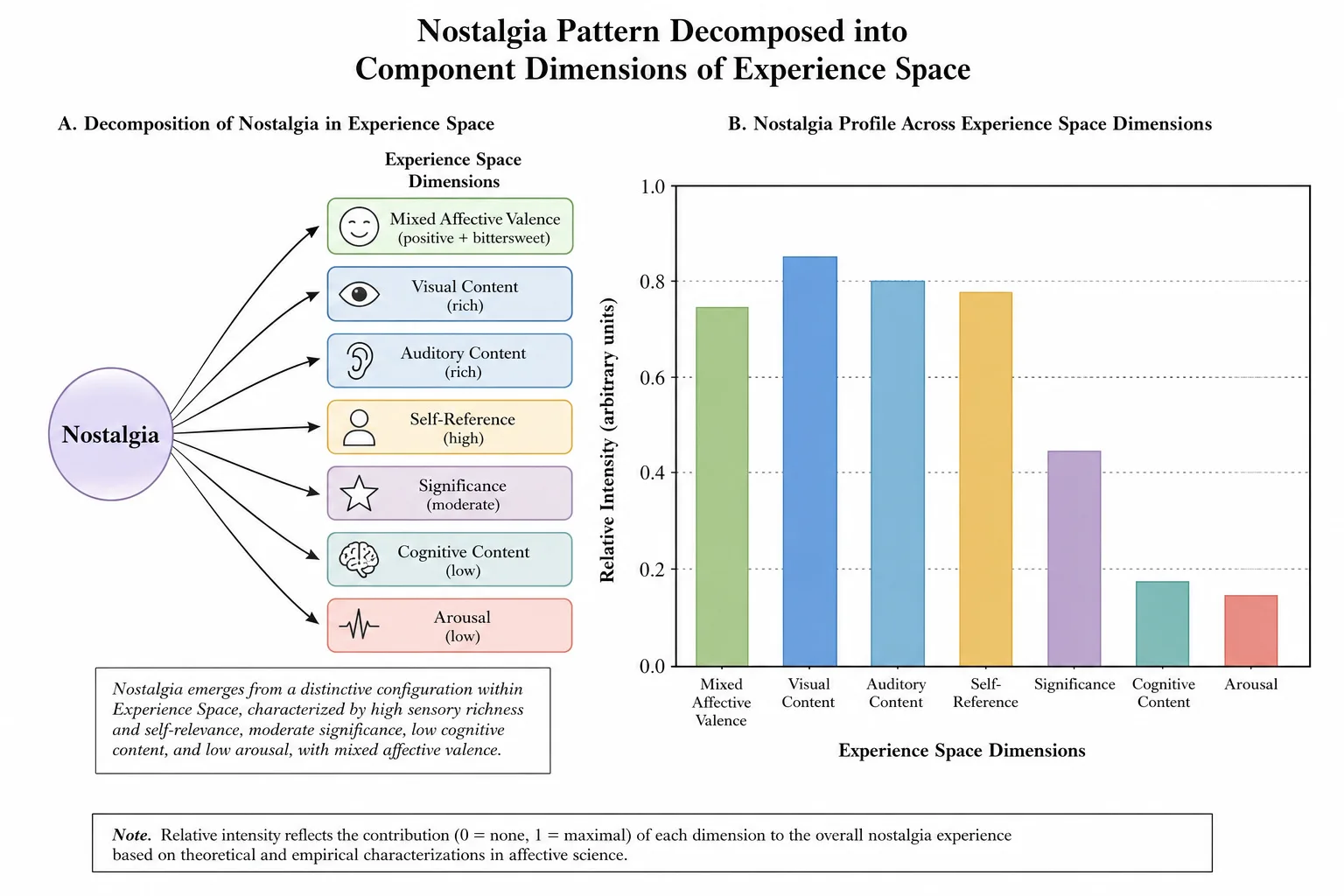
Nostalgia
Nostalgia as a pattern decomposes approximately as: strong Self-reference (the experience is referred to one’s own past), Episodic memory engagement (specific past events recalled), bittersweet Affective valence (mixed positive and negative - pleasant longing combined with awareness of loss), moderate Arousal, and often a specific kind of Significance directed at the recalled period. The Affective component is not pure positive or pure negative; it is the specific mixed valence the construct picks out.
The test (Tool 4): complete disruption of episodic memory access eliminates nostalgia. The neurologist Thorsten Bartsch and colleagues [40] (2011) showed in PNAS that CA1 neurons in the human hippocampus are critical for autobiographical memory and mental time travel; without them, the temporal self-projection that nostalgia requires is impossible. The psychologists Constantine Sedikides and Tim Wildschut [41] (2025) reviewed in Advances in Experimental Social Psychology the psychological mechanisms of nostalgia and its dependence on accessible autobiographical memory. A qualification: Ismail et al. (2018) showed that dementia patients with partial memory loss still experience nostalgia from their preserved memories, so it is complete disruption of episodic memory that eliminates nostalgia, not any partial impairment. Where episodic memory is absent, there is no nostalgia; where fragments remain, nostalgia can still anchor to them. Within an intact mind, altering the Affective valence - making the recalled period feel only positive, or only negative - shifts the experience out of nostalgia into either pure positive recollection or pure regret. Reducing self-reference (memories that are not personally one’s own) shifts the experience into something more like historical curiosity. Each component is necessary; their conjunction at specific values is what nostalgia is.
Khozai implication. Content that engages nostalgia is content that triggers self-referential episodic memory with bittersweet affect - period-specific imagery, music tied to a developmental window, narrative cues that index a recalled era. The framework’s reading of “this reminded me of my dad” or “this took me back” is as a confirmation that the predicted pattern (Self-reference + Episodic memory + bittersweet Affective valence) was activated, which is one of the validation signals Chapter 6 will pick up under self-report extraction. Measurement note: Self-reference sits at higher confidence (mPFC, cortical); Episodic memory sits at mixed confidence (hippocampus, deep medial temporal). Nostalgia is therefore partially in and partially out of TRIBE v2’s readable range.
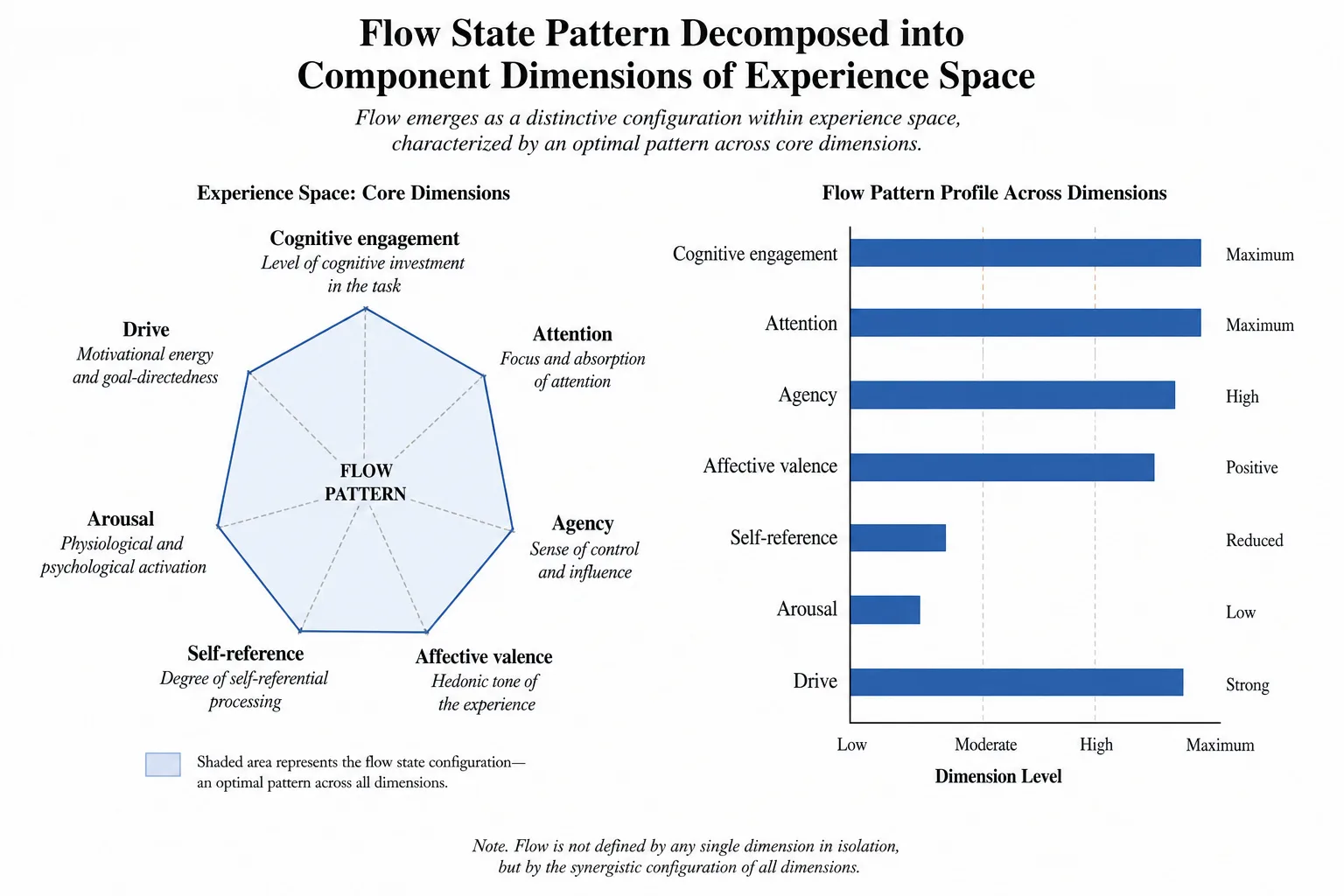
Awe
Awe as a pattern decomposes approximately as: high Significance (the felt sense of importance - something vast, beyond ordinary scale), specific Cognitive content related to perceived vastness (physical, social, intellectual, or moral), Affective valence that is typically positive but can include fear (the “terror” component of awe-as-overwhelm), elevated Arousal, and a characteristic alteration of Self-reference - sometimes called “small self,” in which the experiencing mind feels reduced relative to the perceived vast object.
The test (Tool 4): removing the Significance component (by re-framing the stimulus as ordinary) eliminates awe even with the rest of the configuration preserved. Removing the perceptual or cognitive vastness (by familiarizing the stimulus) does the same. Altering the Self-reference component shifts the experience toward either ordinary admiration (no small-self component) or anxiety (negatively valenced small-self under threat). Each component is necessary.
Khozai implication. Awe-engaging content tends to be content with high spatial or temporal scale (long takes, vast landscapes, slow time-lapse), high perceived stakes (significance cues), and specific affective tone (typically reverent or hushed - neither high-arousal positive like joy nor negative like fear). The pattern view explains why content that hits some but not all of these components fails to produce awe even when it engages high arousal or high affect - it lacks one of the necessary components, and the construct’s behavioral signature is correspondingly absent. Measurement note: Significance and Cognitive content sit at higher confidence (cortical); Arousal sits at lower confidence (brainstem). The “small self” alteration of Self-reference is readable through mPFC deactivation patterns.
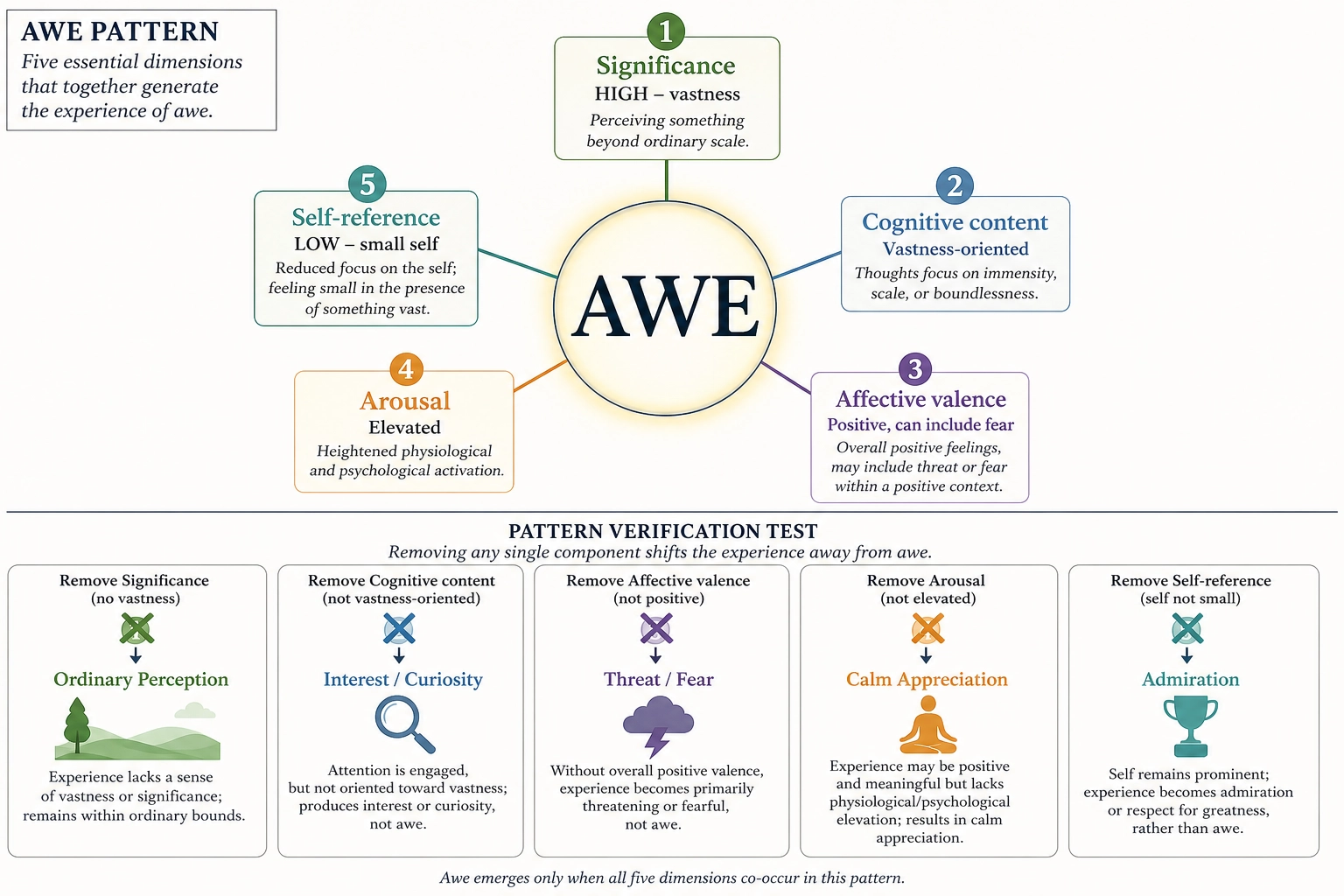
The general claim. In the cases examined, every named psychological construct decomposes into a configuration across dimensions already in the set, with no residual. The claim is falsifiable (Tool 4): a construct that cannot be reconstructed from the dimensions would force a revision of the dimension set. No such case has been established in the literature this framework has surveyed, but the test remains open. The fact that the dimensions reproduce psychology’s named constructs as patterns is evidence in favor of the decomposition. It is not proof that the decomposition is complete; 6. addresses why proof, in this domain, is unavailable.
6. The Spanning Question
The framework claims that the dimensions named here span Experience Space - that every moment of human experience can be described as a point in this dimension space, with no residual that the dimensions fail to capture. This claim is structurally falsifiable. It is also structurally unprovable.
The asymmetry follows from the test. Spanning is tested by attempting to find an experience that cannot be described as a configuration across the dimensions. If such an experience is found, the dimension set is incomplete - either a dimension is missing or the resolution is too coarse. One counter-example falsifies the claim of spanning at the current resolution. No number of confirmations proves it: the next experience tested could still be the one that breaks the set. This is the standard epistemic structure of universal claims, and the framework accepts the asymmetry as the price of being honest about a universal claim.
What can be said in favor of the current dimension set is that it has survived the attempts made on it. The lesion literature from the neuroanatomist Korbinian Brodmann [5] forward has been one long, distributed effort to find aspects of experience that resist decomposition - and the result is that experience does decompose, modality by modality, faculty by faculty, as a finite catalog of separable components. The Pattern Verification Test (Tool 4) applied to psychology’s named constructs has, in the cases this framework has examined, returned successful decompositions. The structural approach Chapter 2 named - Scope A, the structurally inferable region - is the region of Experience Space the framework operates in, and within Scope A the dimensions named here have not been shown to be insufficient.
What cannot be said is that the set is final. Three reasons.
First, Scope B - qualia - is acknowledged as real and not characterized by this framework. Whether the structural decomposition Scope A captures is a complete description of experience depends in part on what the relationship between Scope A and Scope B turns out to be. If the qualitative character of experience adds dimensions of structure that the lesion methods cannot reach, the spanning claim within Scope A could be correct while the broader claim about Experience Space as a whole remained open. This framework does not adjudicate that question; it states the boundary explicitly.
Second, the lesion literature, however extensive, is finite. It is constrained by what damage occurs in human neurology, what surgeries are performed, what patient populations are studied, and what the field has thought to look for. Selective eliminations that have not yet been observed remain possible. New dissociations have been added to the literature in recent decades - the splitting of the visual modality into dedicated areas for color (V4, achromatopsia), motion (MT/V5, akinetopsia), face recognition (FFA, prosopagnosia), and word recognition (VWFA, pure alexia) is largely a development of the second half of the twentieth century and after. The dimension set as named here is the framework’s current best decomposition. It is offered as the best-supported set, not as the final word.
Third, the concept of “experience” itself sits at the edge of what is operationally tractable. The framework operates on Scope A - the structural, decomposable, hardware-mappable aspect of experience - because that is where the methods reach. For the rest of experience, the framework defers. The deferral is not a defect of this framework specifically; it is the deferral every empirical science makes at the edge of its measurement.
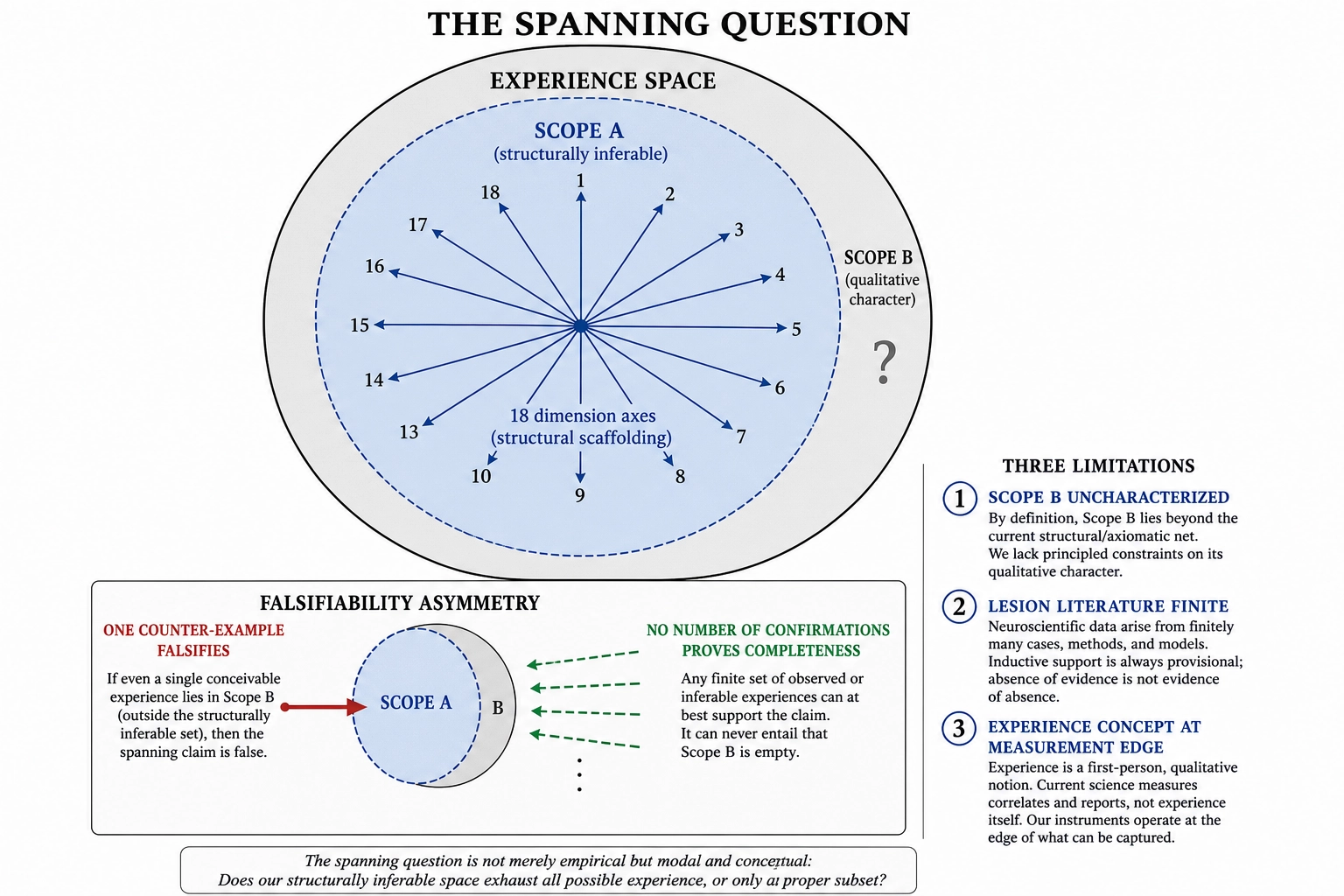
A design consequence deserves stating. The dimension set deliberately over-specifies Experience Space relative to what screen-mediated content can engage. Five of the ten sensory modalities (Tactile, Proprioceptive, Vestibular, Olfactory, Gustatory) are absent or indirect in video content. They are included for three reasons. First, over-specification prevents misattribution: a viewer self-report of “I felt it in my gut” should map to the Interoceptive dimension, not be collapsed into Affective or Arousal because the framework lacked the right axis. Second, it keeps the door open for content modalities that engage those dimensions more directly - immersive VR, haptic interfaces, scent-enabled media - without requiring a structural revision of Experience Space. Third, it ensures the spanning claim is defined by neurology (what the brain can produce) rather than by current technology (what screens can deliver). A framework that excluded dimensions because today’s measurement context does not engage them would need to be re-derived every time the measurement context changes.
What this does NOT say. The spanning claim does not assert that the current dimension set is complete - it asserts that the set has not yet been falsified. It does not assert that Scope B (qualitative character) is covered - the claim applies only within Scope A. It does not assert that all dimensions are equally well-supported - the evidence ratings (Strong, Moderate, Preliminary) and confidence tiers (higher, lower, mixed) state the quality of support for each. It does not assert that the set will never need revision - it asserts that revision will be evidence-driven (a new selective elimination that the current set cannot accommodate) rather than speculative.
Conclusion
This chapter identified the dimensions of human experience and showed the evidence that earns each one its place.
The method is selective elimination: damage a neural structure, observe what disappears from experience, verify that the rest survives. Four formal tools organize that evidence. The Dissociation Test (Tool 1) establishes independence between dimensions. The Atomicity Test (Tool 2) confirms that each dimension is irreducible - not a combination of others, independently variable, and served by dedicated hardware from Chapter 3’s inventory. The Hierarchy Test (Tool 3) nests finer dimensions inside coarser ones. The Pattern Verification Test (Tool 4) shows that psychology’s named constructs - anxiety, flow, nostalgia, awe - decompose into configurations across these dimensions with no residual, confirming the dimensions’ explanatory reach without inflating their count.
The result is a three-level decomposition. At Resolution Level 1, experience separates into five broadest aspects: Sensory, Affective, Cognitive, Motivational, and Bodily. All five carry Strong evidence ratings; only Motivational earns a full double dissociation (wanting versus liking, dopamine versus opioid pathways). At Resolution Level 2 - the framework’s default operating resolution - these five expand to eighteen dimensions: ten sensory modalities and eight non-sensory dimensions (Drive, Hedonic, Arousal, Attention, Agency, Social cognition, Self-reference, Significance). Each has named eliminating evidence, a specific neural substrate, an evidence rating, and a confidence tier. At Resolution Level 3, individual modalities subdivide further - vision into seven sub-dimensions (color, motion, faces, places, objects, words, spatial), audition into four, cognition into four, affect into two - reaching thirty-one enumerated dimensions in total, each with its own selective elimination, with the set open to growth as new dissociations are discovered.
These eighteen dimensions are the axes of Ve - the experiential state vector defined in Chapter 2’s architecture. Of the eighteen, eleven sit at higher confidence (cortical surface, directly readable by TRIBE v2), four at lower confidence (subcortical, inferred but not directly predicted), and three at mixed confidence (cortical endpoint readable, subcortical driver not). The confidence tiers are inherited from Chapter 3’s hardware classification, not assigned by judgment.
Two constraints carry forward. First, the entire decomposition operates within Scope A - the structurally inferable region of Experience Space. Scope B (qualitative character) is real, acknowledged, and not characterized here. Second, the spanning claim - that these dimensions cover all of Scope A - is structurally falsifiable but structurally unprovable. One counter-example (an experience that resists decomposition into the current set) would force revision. No number of confirmations can prove completeness. The dimension set is offered as the best-supported decomposition the evidence currently yields, not as the final word.
This is the experiential architecture. Chapter 5 builds the measurement system on top of it: how Khozai maps content features to Ve values, how TRIBE v2’s cortical predictions become dimension-level engagement estimates, and what the confidence tiers mean in practice for which dimensions the framework can measure directly and which it must infer.
Bibliography
[1] Adolphs, R., Tranel, D., Damasio, H. & Damasio, A. “Fear and the human amygdala.” J. Neurosci. 15(9):5879-5891, 1995. [PEER-REVIEWED] - Used in: 2. Affective (patient SM, bilateral amygdala, selective fear loss); 4. Within Affect (Fear)
[2] Aston-Jones, G. & Cohen, J.D. “An integrative theory of locus coeruleus-norepinephrine function.” Annual Review of Neuroscience 28:403-450, 2005. [PEER-REVIEWED] - Used in: 3. Arousal (locus coeruleus refinement of RAS model)
[3] Berridge, K.C. & Robinson, T.E. “What is the role of dopamine in reward: hedonic impact, reward learning, or incentive salience?” Brain Research Reviews 28(3):309-369, 1998. [PEER-REVIEWED] - Used in: 2. Motivational (wanting-liking double dissociation); 3. Drive and Hedonic
[4] Broca, P. “Remarques sur le siege de la faculte du langage articule.” Bulletin de la Societe Anatomique de Paris 6:330-357, 1861. [PEER-REVIEWED] - Used in: 4. Within Cognition (Speech production, Broca’s aphasia)
[5] Brodmann, K. Vergleichende Lokalisationslehre der Grosshirnrinde. Leipzig: Johann Ambrosius Barth, 1909. [PEER-REVIEWED] - Used in: 6. Spanning (lesion literature history)
[6] Calder, A.J., Keane, J., Manes, F., Antoun, N. & Young, A.W. “Impaired recognition and experience of disgust following brain injury.” Nature Neuroscience 3(11):1077-1078, 2000. [PEER-REVIEWED] - Used in: 4. Within Affect (Disgust, selective insular lesion)
[7] Clarke, S., Bellmann, A., Meuli, R.A., Assal, G. & Steck, A.J. “Auditory agnosia and auditory spatial deficits following left hemispheric lesions.” Brain 123(2):261-279, 2000. [PEER-REVIEWED] - Used in: 4. Within Audition (Environmental sound recognition)
[8] Cole, J. Pride and a Daily Marathon. MIT Press, 1995. [BOOK] - Used in: 2. Bodily (patient IW, proprioceptive loss); 3. Proprioceptive
[9] Corbetta, M. & Shulman, G.L. “Control of goal-directed and stimulus-driven attention in the brain.” Nature Reviews Neuroscience 3:201-215, 2002. [PEER-REVIEWED] - Used in: 3. Attention (dorsal attention network)
[10] Craig, A.D. “How do you feel? Interoception: the sense of the physiological condition of the body.” Nature Reviews Neuroscience 3:655-666, 2002. [PEER-REVIEWED] - Used in: 3. Interoceptive (anterior insula as cortical site for interoceptive awareness)
[11] Csikszentmihalyi, M. Flow: The Psychology of Optimal Experience. Harper & Row, 1990. [BOOK] - Used in: 5. Flow (flow state characterization, challenge-skill balance)
[12] Dehaene, S. & Cohen, L. “The unique role of the visual word form area in reading.” Trends in Cognitive Sciences 15(6):254-262, 2011. [PEER-REVIEWED] - Used in: 4. Within Vision (Word recognition, VWFA, pure alexia)
[13] Epstein, R. & Kanwisher, N. “A cortical representation of the local visual environment.” Nature 392:598-601, 1998. [PEER-REVIEWED] - Used in: 4. Within Vision (Place and scene recognition, PPA)
[14] Farah, M.J. Visual Agnosia: Disorders of Object Recognition and What They Tell Us About Normal Vision. MIT Press, 1990. [BOOK] - Used in: 4. Within Vision (Object recognition, visual agnosia)
[15] Feinstein, J.S., Adolphs, R., Damasio, A. & Tranel, D. “The human amygdala and the induction and experience of fear.” Current Biology 21(1):34-38, 2011. [PEER-REVIEWED] - Used in: 2. Affective (patient SM, extended fear studies)
[16] Haggard, P. “Sense of agency in the human brain.” Nature Reviews Neuroscience 18:196-207, 2017. [PEER-REVIEWED] - Used in: 3. Agency (angular gyrus, SMA, sense of agency)
[17] Hodges, J.R., Patterson, K., Oxbury, S. & Funnell, E. “Semantic dementia: progressive fluent aphasia with temporal lobe atrophy.” Brain 115(6):1783-1806, 1992. [PEER-REVIEWED] - Used in: 4. Within Cognition (Semantic knowledge, semantic dementia)
[18] Kanwisher, N., McDermott, J. & Chun, M.M. “The fusiform face area: a module in human extrastriate cortex specialized for face perception.” J. Neurosci. 17(11):4302-4311, 1997. [PEER-REVIEWED] - Used in: 4. Within Vision (Face recognition, FFA, prosopagnosia)
[19] Luria, A.R. Higher Cortical Functions in Man. Basic Books, 1966. [BOOK] - Used in: 2. Cognitive (dysexecutive syndrome, early lesion literature)
[20] Mesulam, M.M. “A cortical network for directed attention and unilateral neglect.” Annals of Neurology 10(4):309-325, 1981. [PEER-REVIEWED] - Used in: 4. Within Vision (Spatial awareness, hemispatial neglect)
[21] Moruzzi, G. & Magoun, H.W. “Brain stem reticular formation and activation of the EEG.” Electroencephalography and Clinical Neurophysiology 1(4):455-473, 1949. [PEER-REVIEWED] - Used in: 3. Arousal (reticular activating system characterization)
[22] Nakamura, J. & Csikszentmihalyi, M. “The concept of flow.” In Handbook of Positive Psychology, Oxford University Press, 2002. [PEER-REVIEWED] - Used in: 5. Flow (flow state in content engagement)
[23] Northoff, G., Heinzel, A., de Greck, M., Bermpohl, F., Dobrowolny, H. & Panksepp, J. “Self-referential processing in our brain - a meta-analysis of imaging studies on the self.” NeuroImage 31(1):440-457, 2006. [PEER-REVIEWED] - Used in: 3. Self-reference (mPFC as self-referential processing site)
[24] Peretz, I., Champod, A.S. & Hyde, K.L. “Varieties of musical disorders: the Montreal Battery of Evaluation of Amusia.” Annals of the New York Academy of Sciences 999:58-75, 2002. [PEER-REVIEWED] - Used in: 4. Within Audition (Music perception, amusia)
[25] Saxe, R. & Kanwisher, N. “People thinking about thinking people: the role of the temporo-parietal junction in theory of mind.” NeuroImage 19(4):1835-1842, 2003. [PEER-REVIEWED] - Used in: 3. Social cognition (TPJ, theory of mind)
[26] Scoville, W.B. & Milner, B. “Loss of recent memory after bilateral hippocampal lesions.” J. Neurol. Neurosurg. Psychiatry 20(1):11-21, 1957. [PEER-REVIEWED] - Used in: 2. Cognitive (patient HM); 4. Within Cognition (Episodic memory)
[27] Seeley, W.W., Menon, V., Schatzberg, A.F., Keller, J., Glover, G.H., Kenna, H., Reiss, A.L. & Greicius, M.D. “Dissociable intrinsic connectivity networks for salience processing and executive control.” J. Neurosci. 27(9):2349-2356, 2007. [PEER-REVIEWED] - Used in: 3. Significance (salience network)
[28] Shallice, T. “Specific impairments of planning.” Philosophical Transactions of the Royal Society of London B 298(1089):199-209, 1982. [PEER-REVIEWED] - Used in: 2. Cognitive (dysexecutive syndrome); 4. Within Cognition (Planning and sequencing)
[29] Stuss, D.T. & Benson, D.F. The Frontal Lobes. Raven Press, 1986. [BOOK] - Used in: 2. Cognitive (dysexecutive syndrome, prefrontal damage)
[30] Zatorre, R.J. & Penhune, V.B. “Spatial localization after excision of human auditory cortex.” J. Neurosci. 21(16):6321-6328, 2001. [PEER-REVIEWED] - Used in: 4. Within Audition (Sound localization, planum temporale)
[31] Zeki, S. “A century of cerebral achromatopsia.” Brain 113(6):1721-1777, 1990. [PEER-REVIEWED] - Used in: 4. Within Vision (Color, V4, achromatopsia)
[32] Wernicke, C. Der aphasische Symptomencomplex. Breslau: Cohn & Weigert, 1874. [PEER-REVIEWED] - Used in: 4. Within Audition (Speech comprehension, Wernicke’s aphasia)
[33] Zihl, J., von Cramon, D. & Mai, N. “Selective disturbance of movement vision after bilateral brain damage.” Brain 106(2):313-340, 1983. [PEER-REVIEWED] - Used in: 4. Within Vision (Motion, MT/V5, akinetopsia)
[34] Dunn, J.C. & Kirsner, K. “Discovering functionally independent mental processes: The principle of reversed association.” Psychological Review 95(1):91-101, 1988. [PEER-REVIEWED] - Used in: 1. Method (dissociation method critique)
[35] Fernandez, A. et al. “Transcranial magnetic stimulation to frontal but not occipital cortex disrupts endogenous attention.” PNAS, 120(10):e2219635120, 2023. [PEER-REVIEWED] - Used in: 3. Attention (TMS to right frontal eye field selectively disrupts voluntary attention while preserving stimulus-driven attention)
[36] Seeley, W.W. “Anterior insula degeneration in frontotemporal dementia.” Brain Structure and Function, 214(5-6):465-475, 2010. [PEER-REVIEWED] - Used in: 3. Significance (bvFTD patients with frontoinsular degeneration lose the felt sense that things matter while retaining language and visuospatial function)
[37] Stendardi, D., Biscotto, F., Bertossi, E. & Ciaramelli, E. “Present and future self in memory: the role of vmPFC in the self-reference effect.” Social Cognitive and Affective Neuroscience, 16(12):1205-1213, 2021. [PEER-REVIEWED] - Used in: 3. Self-reference (vmPFC lesion patients showed abolished self-reference effect in memory while brain-damaged controls retained it)
[38] Marr, C. & Theeuwes, J. “Flow experience and the mobilization of attentional resources.” Cognitive, Affective, & Behavioral Neuroscience, 18(4):810-823, 2018. [PEER-REVIEWED] - Used in: 5. Flow (flow depends on complete mobilization of attentional resources in frontoparietal networks)
[39] Harris, D.J., Vine, S.J. & Wilson, M.R. “Neurocognitive mechanisms of the flow state.” Progress in Brain Research, 234:221-243, 2017. [REVIEW] - Used in: 5. Flow (flow requires sustained frontoparietal engagement; disrupting attention breaks the state)
[40] Bartsch, T. et al. “CA1 neurons in the human hippocampus are critical for autobiographical memory, mental time travel, and autonoetic consciousness.” PNAS, 108(42):17562-17567, 2011. [PEER-REVIEWED] - Used in: 5. Nostalgia (hippocampal CA1 neurons required for the temporal self-projection nostalgia depends on)
[41] Sedikides, C. & Wildschut, T. “On the Nature of Nostalgia: A Psychological Perspective.” Advances in Experimental Social Psychology, 2025. [REVIEW] - Used in: 5. Nostalgia (nostalgia depends on accessible autobiographical memory; psychological mechanisms review)
[42] Evans, A.H. et al. “Compulsive drug use linked to sensitized ventral striatal dopamine transmission.” Annals of Neurology, 59(5):852-858, 2006. [PEER-REVIEWED] - Used in: 2. Motivational (PET in Parkinson’s patients showing sensitized ventral striatal dopamine release correlated with wanting but not liking)
[43] Berridge, K.C. & Robinson, T.E. “Liking, wanting, and the incentive-sensitization theory of addiction.” American Psychologist, 71(8):670-679, 2016. [REVIEW] - Used in: 2. Motivational (human evidence for wanting-liking dissociation across addiction, Parkinson’s disease, and pharmacological studies)
[44] Ismail, S., Christopher, G., Dodd, E., et al. “Psychological and mnemonic functions of nostalgia in the elderly.” Journal of Aging and Health, 2018. [PEER-REVIEWED] - Used in: 5. Nostalgia (dementia patients with partial memory loss still experience nostalgia from preserved memories)